📅 Published on May 7, 2026 | 🕒 Last updated on June 25, 2026
Why Muscle Anatomy Matters
Skeletal muscles make up about 40% of an adult’s body weight. They work together in groups, contracting and relaxing in specific patterns controlled by the nervous system to create all voluntary movements, from blinking to sprinting. Knowing muscle anatomy is crucial for healthcare professionals when planning surgeries, diagnosing nerve injuries, developing rehab plans, and analyzing movement in sports medicine. For students and fitness professionals, understanding muscle anatomy helps prevent injuries and improve performance.
This guide presents a systematic, region-by-region analysis of all major human muscle groups, validated against current United States clinical guidelines and peer-reviewed evidence.
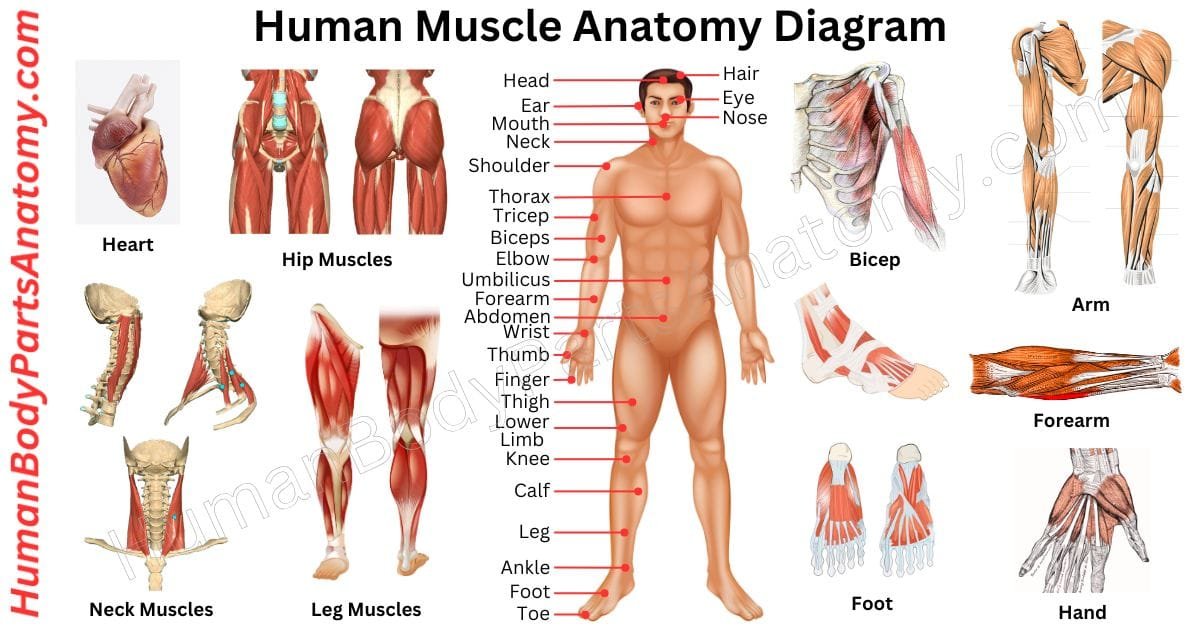
Muscles of Human Body Diagram
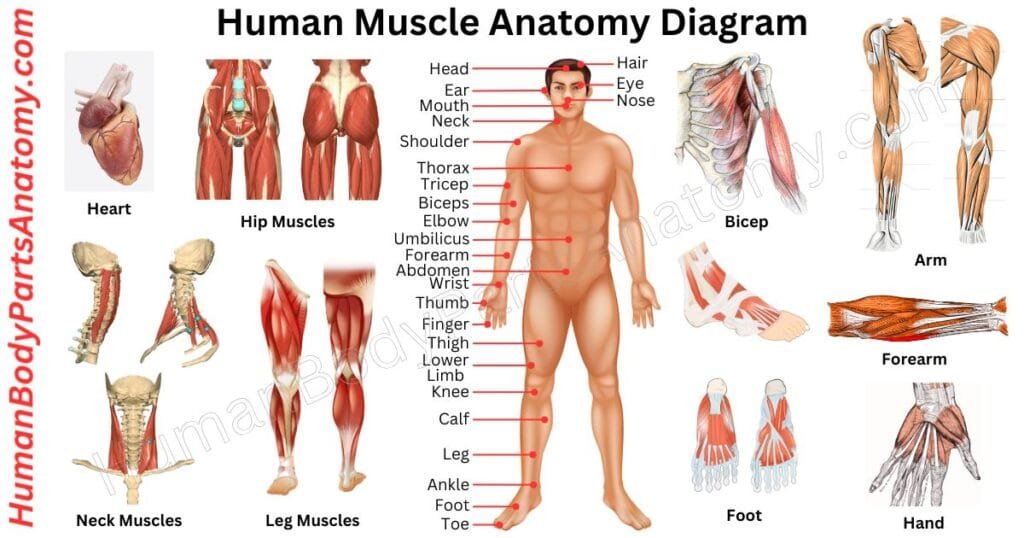
Human Muscle Anatomy
1. Head and Face Muscles
- Muscles of Facial Expression
- Frontalis
- Orbicularis Oculi
- Orbicularis Oris
- Zygomaticus Major
- Buccinator
- Muscles of Mastication (Chewing)
- Masseter
- Temporalis
- Medial Pterygoid
- Lateral Pterygoid
2. Neck Muscles
- Sternocleidomastoid (SCM)
- Platysma
- Scalenes (Anterior, Middle, Posterior)
- Levator Scapulae
3. Shoulder Muscles
- Deltoid
The Rotator Cuff (SITS Muscles)
- Supraspinatus
- Infraspinatus
- Teres Minor
- Subscapularis
4. Upper Back Muscles
- Trapezius
- Rhomboid Major and Minor
- Latissimus Dorsi
5. Chest Muscles
- Pectoralis Major
- Pectoralis Minor
- Serratus Anterior
- Intercostal Muscles
6. Arm Muscles
- Upper Arm
- Biceps Brachii
- Triceps Brachii
- Brachialis
- Coracobrachialis
- Forearm Muscles
- Anterior Compartment (Flexor Group)
- Posterior Compartment (Extensor Group)
7. Core (Abdominal) Muscles
- Rectus Abdominis
- External Oblique
- Internal Oblique
- Transversus Abdominis (TrA)
8. Lower Back Muscles
- Erector Spinae
- Multifidus
- Quadratus Lumborum (QL)
9. Hip Muscles
- Gluteus Maximus
- Gluteus Medius
- Gluteus Minimus
- Iliopsoas (Iliacus + Psoas Major)
10. Thigh Muscles
- Anterior Thigh: Quadriceps Femoris
- Rectus Femoris
- Vastus Lateralis
- Vastus Medialis
- Vastus Intermedius
- Posterior Thigh: Hamstrings
- Biceps Femoris
- Semitendinosus
- Semimembranosus
- Inner Thigh: Adductor Group
- Adductor Longus
- Adductor Brevis
- Adductor Magnus
- Gracilis
11. Lower Leg Muscles
- Posterior Leg: Calf Group
- Gastrocnemius
- Soleus
- Plantaris
- Anterior Leg
- Tibialis Anterior
- Extensor Digitorum Longus
- Lateral Leg: Fibular (Peroneal) Group
- Fibularis (Peroneus) Longus
- Fibularis (Peroneus) Brevis
1. Head and Face Muscles
Muscles of Facial Expression
The muscles of facial expression are anatomically distinct because they insert directly into the dermis instead of bone, enabling precise movement of the overlying skin.
All facial muscles are innervated by the facial nerve (cranial nerve VII). This is clinically significant because a single lesion can affect multiple muscles throughout the face simultaneously.
1. Frontalis
This muscle originates from the galea aponeurotica and inserts into the skin of the forehead and eyebrows. The frontalis elevates the eyebrows and produces horizontal forehead creases.
Clinically, its function is among the first to be assessed in cases of cranial nerve VII palsy, as loss of forehead wrinkling on the affected side is a key indicator.
2. Orbicularis Oculi
This ring-shaped muscle surrounds the eye and has three parts: orbital, preseptal, and pretarsal. The orbital part closes the eye tightly, like when you squint, while the palpebral part controls blinking.
Weakness of the orbicularis oculi results in lagophthalmos, or incomplete eyelid closure, which increases the risk of corneal exposure injury.
3. Orbicularis Oris
Rather than forming a single ring muscle, the orbicularis oris consists of an interlocking network of fibers derived from multiple surrounding facial muscles.
It compresses and protrudes the lips and is essential for intelligible speech, whistling, and oral containment during chewing.
4. Zygomaticus Major
This muscle extends obliquely from the zygomatic bone to the angle of the mouth, this muscle draws the lip superolaterally during smiling.
It is the primary muscle examined in research on the “Duchenne smile.” Genuine smiling involves involuntary co-contraction with the orbicularis oculi, whereas posed smiles often do not.
5. Buccinator
The buccinator forms the deep muscular layer of the cheek. It compresses the cheek against the molar teeth during chewing and is traversed by the parotid duct. This muscle is important in dental anesthesia, maxillofacial surgery, and parotid gland pathology.
Muscles of Mastication (Chewing)
The four primary muscles responsible for mastication receive innervation from the mandibular branch of the trigeminal nerve (cranial nerve V3). These muscles facilitate temporomandibular joint (TMJ) movement, enabling the complex actions required for chewing and speaking.
The masseter originates from the zygomatic arch and inserts onto the angle and ramus of the mandible. Relative to its size, it is the most powerful muscle involved in jaw closure.
Hypertrophy of the masseter muscle, often resulting from chronic bruxism or frequent jaw clenching, can lead to a broader facial appearance. This condition is a common indication for botulinum toxin (Botox) injections in both cosmetic and therapeutic contexts.
1. Temporalis
This broad, fan-shaped muscle covers the temporal fossa and inserts via a tendon into the coronoid process of the mandible. The anterior fibers elevate the jaw, while the posterior fibers retract the protruded mandible.
During temporomandibular joint assessment, clinicians routinely palpate the temporalis muscle at the temple while the patient clenches the jaw. Tenderness in this region is a characteristic finding in temporomandibular disorder (TMD).
2. Medial Pterygoid
This muscle works alongside the masseter in a sling-like arrangement beneath the mandible. The medial pterygoid elevates and protrudes the jaw and also contributes to the mediolateral grinding motions of chewing.
3. Lateral Pterygoid
Unlike the other muscles of mastication, the lateral pterygoid depresses the mandible (opens the jaw) when both sides contract bilaterally. Unilateral contraction causes deviation of the jaw toward the contralateral side.
The lateral pterygoid primarily advances the jaw and plays a critical role in the function of the temporomandibular joint disc. The superior head attaches to the articular disc, directly contributing to temporomandibular joint dysfunction.
2. Neck Muscles
Sternocleidomastoid (SCM)
This primary anterior neck muscle runs obliquely from the manubrium of the sternum and medial clavicle to the mastoid process of the temporal bone.
Unilateral contraction results in ipsilateral neck tilt and contralateral face rotation, a movement pattern used in the clinical assessment of torticollis (wry neck).
Bilateral contraction flexes the neck against gravity. The SCM serves as a key landmark for identifying the jugular venous system, carotid pulse, and anterior triangle of the neck.
Platysma
This thin, sheet-like subcutaneous muscle spans the lower face and anterior neck. It depresses the mandible and lower lip and tenses the overlying skin.
With age-related tissue laxity, the platysma develops vertical banding, known as “platysmal bands,” which are often targeted in lower face and neck rejuvenation procedures.
Scalenes (Anterior, Middle, Posterior)
These muscles originate from the cervical transverse processes and insert onto ribs 1 and 2. They are the primary accessory muscles for deep inhalation, elevating the upper rib cage when the cervical spine is stabilized.
The scalenes also help bend and tilt the neck to the side. In medicine, the space between the anterior and middle scalenes, called the scalene triangle, is important because it contains the brachial plexus and subclavian artery.
If the scalene triangle becomes crowded by muscle growth, spasms, or unusual bands, it can press on these nerves and blood vessels. This can lead to thoracic outlet syndrome (TOS), which causes arm pain, tingling, or problems with blood flow.
Levator Scapulae
This muscle extends from the transverse processes of C1 to C4 to the superior angle of the medial scapular border. It elevates the scapula and assists in downward rotation.
It is a common site for myofascial trigger point formation in the neck-shoulder region, especially in individuals who maintain prolonged cervical flexion during computer or smartphone use.
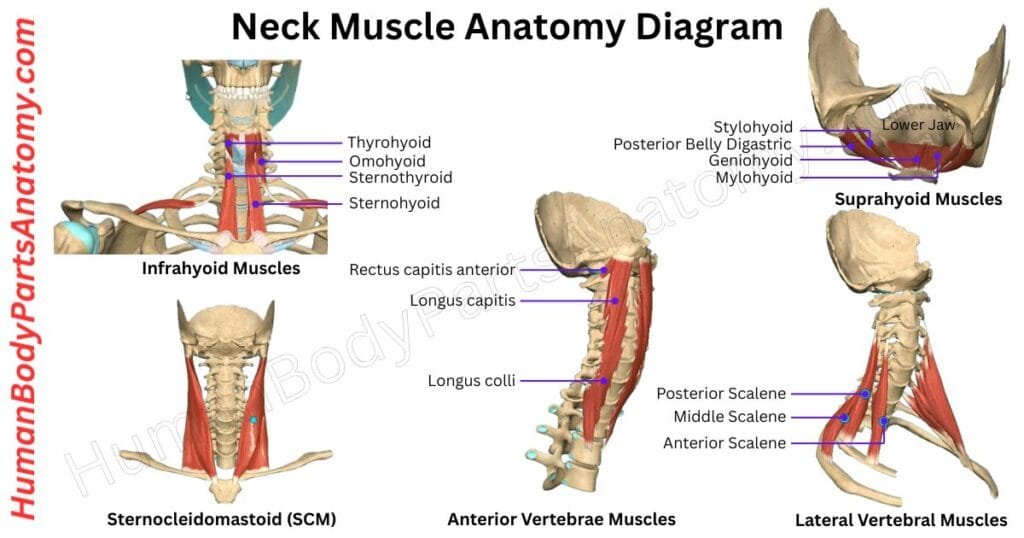
Read More – Neck Muscle Anatomy: Complete Guide with Parts, Names & Diagram
3. Shoulder Muscles
Deltoid: The deltoid surrounds the shoulder girdle and serves as the primary mover of the glenohumeral joint. Its three parts have distinct roles: the anterior head flexes and internally rotates the arm, the middle head abducts it, and the posterior head extends and externally rotates it.
The deltoid is innervated by the axillary nerve (C5–C6), which exits the posterior cord of the brachial plexus and winds around the surgical neck of the humerus.
Anterior shoulder dislocation, the most common large-joint dislocation in emergency departments, directly endangers the axillary nerve. Deltoid weakness after dislocation should prompt clinical nerve assessment.
The Rotator Cuff (SITS Muscles)
The rotator cuff is a group of four important muscles that help move and stabilize the shoulder joint. These muscles keep the humeral head pressed into the shallow socket of the shoulder. Without this support, the shoulder’s wide range of motion would make it unstable.
1. Supraspinatus
It originates in the supraspinous fossa of the scapula and inserts into the superior facet of the greater tuberosity. The supraspinatus initiates the first 15–30 degrees of arm abduction.
It passes beneath the coracoacromial arch — a bony-ligamentous tunnel where impingement is common. The supraspinatus is the most frequently torn rotator cuff tendon, particularly in individuals with overhead occupational or athletic demands.
Clinical tests include the Hawkins-Kennedy test (for impingement) and the empty-can test (for supraspinatus integrity).
2. Infraspinatus
It occupies the infraspinous fossa and inserts on the middle facet of the greater tuberosity. The infraspinatus is the primary external rotator of the shoulder. External rotation strength testing and the external rotation lag sign are used to assess its integrity.
The AAOS 2025 CPG notes that clinical examination alone is insufficient for definitive rotator cuff tear diagnosis and that MRI, MR arthrography (MRA), CT, and ultrasound are useful adjuncts — with a strong evidence recommendation supporting their role in clinical decision-making.
3. Teres Minor
A small, cylindrical muscle below the infraspinatus, teres minor also externally rotates and adducts the arm. It shares innervation (axillary nerve) with the deltoid, and both are affected together in axillary nerve injuries.
4. Subscapularis
The only rotator cuff muscle on the anterior (costal) surface of the scapula, the subscapularis internally rotates and adducts the arm while protecting the anterior capsule of the shoulder joint.
It is the most powerful of the four rotator cuff muscles. Isolated subscapularis tears are evaluated using the lift-off test (asking the patient to lift the hand away from the lumbar spine) and the belly-press test.
The AAOS 2025 guidelines strongly recommend repairing rotator cuff tears, as healed repairs lead to better patient outcomes than non-surgical treatment or unhealed repairs. This highlights the need for accurate diagnosis and early referral for surgery when needed.
4. Upper Back Muscles
Trapezius
One of the largest and most functionally complex muscles of the posterior trunk, the trapezius spans from the external occipital protuberance and nuchal ligament superiorly to the spinous process of T12 inferiorly, with lateral insertions on the clavicle and scapular spine.
The trapezius has three parts: the upper fibers lift the scapula, the middle fibers pull it toward the spine, and the lower fibers lower it. Working together, these parts help rotate the scapula upward, which is needed to raise your arm above shoulder level without pinching.
The spinal accessory nerve (CN XI) controls the trapezius. If this nerve is damaged during neck surgery or a lymph node biopsy in the back of the neck, it can lead to trapezius palsy. This causes the shoulder blade to stick out, the shoulder to droop, and makes it painful and hard to lift the arm.
Rhomboid Major and Minor
The rhomboids originate from the spinous processes of C7–T5 and insert along the medial border of the scapula. They retract the scapula (adduct it toward the midline), assist with downward rotation, and help press the medial scapular border against the posterior thoracic wall.
Rhomboid weakness, which is common in individuals with sustained forward head and rounded shoulder postures, contributes to scapular dyskinesis and is a frequent rehabilitation target in postural correction programs.
Latissimus Dorsi
The latissimus dorsi (lats) is the broadest muscle of the back, originating from the thoracolumbar fascia, the spinous processes of T7–T12, the posterior iliac crest, and the inferior four ribs.
It inserts via a flat tendon into the intertubercular groove (bicipital groove) of the humerus. Its primary actions are arm adduction, extension, and internal rotation. These combined movements power pull-ups, rowing, and swimming strokes.
The latissimus is also a key contributor to trunk stability and is used as a pedicled muscle flap in reconstructive breast surgery following mastectomy.
5. Chest Muscles
Pectoralis Major
The largest anterior chest muscle has two distinct heads with different actions. The clavicular head (superior portion) flexes and horizontally adducts the arm. The sternocostal head (inferior portion) adducts the arm and internally rotates it.
Together, they are the primary drivers of pressing and pushing movements. The pectoralis major is innervated by both the medial and lateral pectoral nerves (C5–T1).
Poland syndrome — congenital unilateral absence of the sternal head of the pectoralis major, often associated with ipsilateral hand anomalies — is a recognized clinical entity.
In bodybuilding, complete pectoralis major tendon rupture at the humeral insertion occurs during heavy bench pressing and requires surgical repair.
Pectoralis Minor
The pectoralis minor originates from ribs 3–5 and inserts into the coracoid process of the scapula. It anteriorly tilts and protracts the scapula.
Tightness of the pectoralis minor — common in individuals with chronic forward shoulder posture — creates anterior scapular tilt that reduces subacromial space and contributes to rotator cuff impingement.
Stretching of the pectoralis minor is a standard component of shoulder impingement and rotator cuff rehabilitation programs.
Serratus Anterior
It originates from the superolateral surfaces of ribs 1–8 (and sometimes rib 9) and inserts along the costal surface of the medial scapular border. The serratus anterior pulls the scapula forward and upward around the thorax.
It is the primary muscle maintaining the scapula flush against the posterior chest wall and is essential for scapular upward rotation during arm elevation.
Intercostal Muscles
The three layers of intercostal muscles — external, internal, and innermost — occupy the intercostal spaces between ribs. The external intercostals raise the ribs during active inhalation; the internal intercostals depress the ribs during forced exhalation.
Their activity is clinically observable. Intercostal retractions, which are the inward drawing of the skin between the ribs during inhalation, indicate increased work of breathing and are a key finding in respiratory distress assessment.
6. Arm Muscles
The muscles of the arm are divided into two main regions: the upper arm and the forearm. Each region contains different muscle groups that work together to support movement, strength, and flexibility of the arm, wrist, and hand.
Upper Arm
1. Biceps Brachii
The biceps has two heads: the long head arises from the supraglenoid tubercle of the scapula (and travels through the bicipital groove of the humerus), while the short head originates from the coracoid process.
Primary functions include forearm supination and elbow flexion; it also assists with shoulder flexion. Rupture of the long head tendon — producing the characteristic “Popeye deformity” (a balled-up muscle belly visible in the distal arm) — is common in middle-aged adults and may be managed conservatively or surgically depending on functional demands.
The biceps jerk reflex (eliciting biceps contraction via the tendon) tests the integrity of the C5–C6 nerve roots.
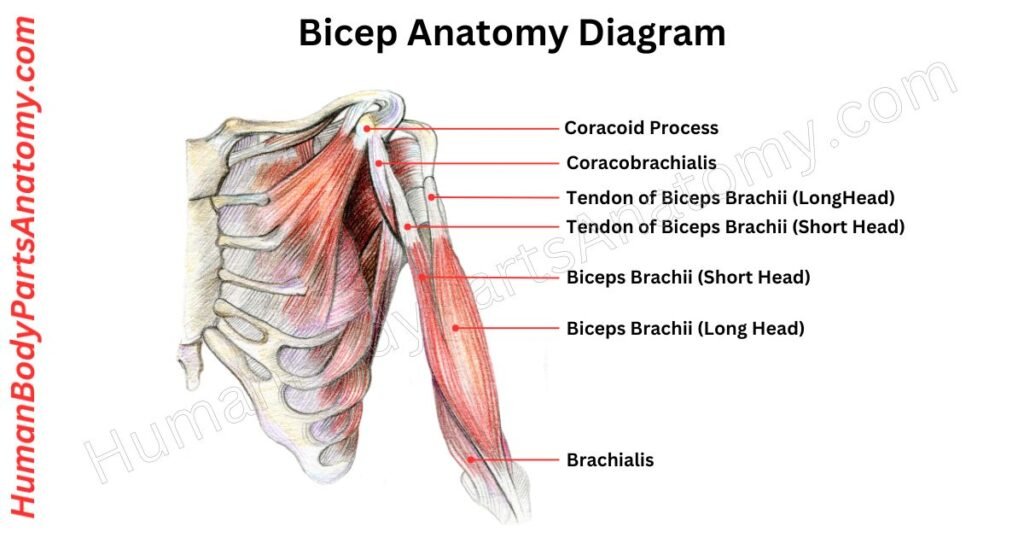
Read More – Ultimate Guide to Bicep Anatomy: Parts, Names, Functions & Diagram
2. Triceps Brachii
With three heads (long, lateral, medial), the triceps is the sole extensor of the elbow. The long head also extends and adducts the arm at the shoulder.
The radial nerve (C7) innervates the triceps, and the triceps jerk reflex tests the C7 root level. The radial nerve is most commonly injured at the spiral groove of the humerus, producing wrist drop and finger extension weakness while typically sparing triceps strength due to its proximal innervation.
3. Brachialis
It originates from the anterior surface of the distal humerus and inserts into the ulnar tuberosity. The brachialis is a pure elbow flexor — unlike the biceps, its force does not change with forearm rotation, making it the most consistent and reliable flexor regardless of position. It is innervated primarily by the musculocutaneous nerve with an additional branch from the radial nerve.
4. Coracobrachialis
This slender muscle runs from the coracoid process to the medial shaft of the humerus. It assists with shoulder flexion and adduction. The musculocutaneous nerve pierces through the coracobrachialis before innervating the anterior arm compartment — compression or injury here can mimic a “C6 radiculopathy” but is distinguishable by the sparing of forearm sensation.
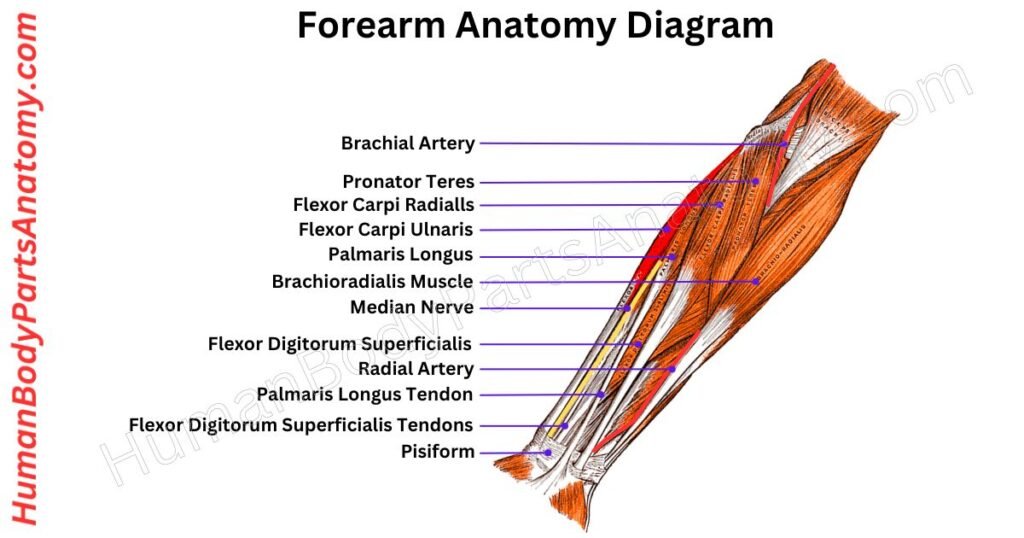
Forearm Muscles
The forearm contains around 20 muscles, grouped into two main compartments—an anterior (front) compartment and a posterior (back) compartment. These muscles work together to control movements of the wrist, hand, and fingers, enabling actions such as gripping, lifting, rotating the forearm, and performing fine motor tasks.
1. Anterior Compartment (Flexor Group)
The flexor compartment controls wrist and finger flexion and forearm pronation. Key muscles include the flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis (FDS — flexes the PIP joints), flexor digitorum profundus (FDP — the only muscle that flexes the distal interphalangeal joints), and the pronator teres. The median nerve and ulnar nerve innervate the compartment’s muscles in complementary territories.
2. Posterior Compartment (Extensor Group)
The extensor compartment is responsible for wrist and digit extension and forearm supination. Notable muscles include the extensor carpi radialis longus and brevis (ECRL, ECRB), extensor digitorum communis, extensor carpi ulnaris, and the supinator.
The common extensor origin at the lateral epicondyle of the humerus is the site of lateral epicondylalgia, commonly known as “tennis elbow,” which primarily affects the ECRB tendon.
This is among the most common upper extremity overuse injuries in both athletic and occupational settings.
Read More – Complete Guide to Forearm Anatomy: Parts, Names, Functions & Diagram
7. Core (Abdominal) Muscles
The four layers of the abdominal wall create a self-contained pressure chamber around the lumbar spine. When co-activated, they generate intra-abdominal pressure that offloads compressive spinal forces — functioning, in effect, as the body’s built-in weightlifting belt.
Rectus Abdominis
These paired, vertically oriented muscles extend from the pubic symphysis to the xiphoid process and the costal cartilages of ribs 5 to 7. They are separated at the midline by the linea alba.
They are the primary muscles responsible for trunk flexion. Tendinous intersections divide each muscle into segments, creating the “six-pack” appearance in lean, trained individuals.
Diastasis recti — abnormal widening of the linea alba — is a clinically important finding in postpartum women and individuals with abdominal obesity, and is an essential consideration before prescribing abdominal strengthening exercises.
External Oblique
The most superficial lateral abdominal muscle has fibers running inferomedially (in the direction of hands-in-front-pockets). It flexes the trunk, laterally bends the spine ipsilaterally, and rotates the trunk contralaterally.
Its aponeurosis contributes to the formation of the inguinal ligament and the anterior rectus sheath — structures central to inguinal hernia anatomy and repair.
Internal Oblique
It is located deep to the external oblique, its fibers run in the opposite, superomedial direction. The internal oblique rotates the trunk to the same side and assists with lateral flexion.
The cross-sectional X-shaped arrangement of the two oblique muscle pairs creates a natural brace that resists torsional spinal loading during rotational movements.
Transversus Abdominis (TrA)
The deepest abdominal layer runs horizontally around the trunk, encircling it like a natural corset.
Unlike the other abdominal muscles, the TrA does not produce visible trunk movement, but activates fractionally before voluntary limb movements to pre-tension the thoracolumbar fascia and stiffen the spine against impending loads.
8. Lower Back Muscles
The erector spinae is a group of muscles and tendons that run vertically from the sacrum up to the skull. It has three parts: the iliocostalis on the outside, the longissimus in the middle, and the spinalis next to the spine.
These muscles help straighten the spine and are important for keeping us upright. Strain in the erector spinae is a common cause of sudden low back pain in the US.
Multifidus
The multifidus runs in short, angled segments from the transverse processes of the lower vertebrae to the spinous processes of the ones above. It helps stabilize each part of the spine by stiffening individual joints when we move or put weight on them, instead of moving the whole trunk.
It is the main deep muscle that stabilizes the back of the spine & works together with the transversus abdominis and pelvic floor as part of the inner unit triad.
Quadratus Lumborum (QL)
It runs from the posterior iliac crest to the 12th rib and transverse processes of L1–L4. The QL laterally flexes the lumbar spine, hikes the hip, and anchors the 12th rib as a fixed point for diaphragmatic contraction during breathing.
Because it connects the pelvis and the chest, the QL is often missed as a cause of ongoing lower back and back-of-the-hip pain. It can also cause pain that feels like nerve pain from the lower back.
Trigger points in the QL often lead to deep, aching pain in the back of the hip bone and the side of the hip.
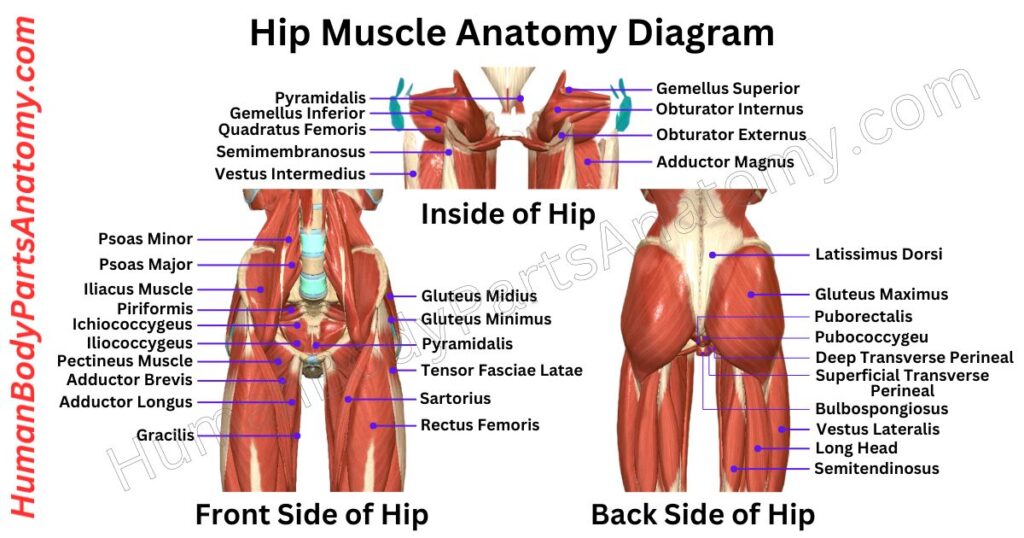
9. Hip Muscles
Gluteus Maximus
The gluteus maximus is the largest muscle in the human body by mass. It originates from the posterior iliac crest, sacrum, and sacrotuberous ligament, inserting into the iliotibial band and gluteal tuberosity of the femur.
It is the main muscle that extends the hip and is also a strong external rotator. This muscle powers explosive lower-body movements like sprinting, climbing stairs, and lifting heavy objects from the floor.
Weakness in the gluteus maximus leads to certain compensations, such as anterior pelvic tilt (which increases lumbar lordosis), too much leaning of the trunk to the opposite side during single-leg stance, and knee valgus collapse during landing. Each of these increases the risk of injury throughout the body’s movement chain.
Gluteus Medius
The gluteus medius is located on the side of the hip, between the iliac crest and the greater trochanter. Its main actions are moving the leg away from the body (abduction) and rotating it inward.
During the single-leg stance phase of walking, the gluteus medius keeps the opposite side of the pelvis from dropping. If it fails, this is called the Trendelenburg sign.
Gluteus Minimus
The gluteus minimus is the smallest and deepest gluteal muscle. It shares its starting point (the outer ilium) and main actions (abduction and internal rotation) with the gluteus medius. These two muscles work together to stabilize the hip.
Tears in the gluteus minimus, which can be seen on MRI, are linked to pain around the greater trochanter and abnormal walking patterns (Arthroscopy, 2024).
Iliopsoas (Iliacus + Psoas Major)
The iliopsoas is the main hip flexor and is made up of two muscles: the iliacus, which comes from the iliac fossa, and the psoas major, which starts at the vertebral bodies and transverse processes of T12 to L5. These muscles join together and attach to the lesser trochanter of the femur.
When the hip is extended, such as when standing, a tight iliopsoas tilts the pelvis forward and increases the curve in the lower back.
This is a common posture problem in people who are inactive and is a major cause of low back pain related to tight hip flexors.
The psoas major is the only muscle that links the lumbar spine to the lower limb. Because of this, its length and how it is activated are very important for the movement and health of the lower back.
Read More – Hip Muscle Anatomy: Complete Guide with Parts, Names, Functions & Diagram
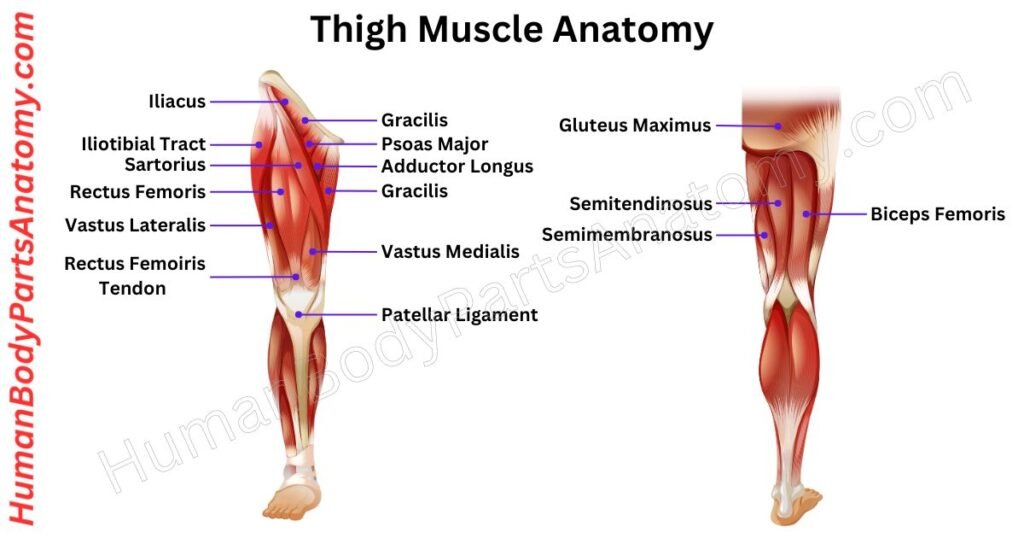
10. Thigh Muscles
Anterior Thigh: Quadriceps Femoris
The four quadriceps muscles converge on a common quadriceps tendon that envelops the patella and continues as the patellar tendon to insert into the tibial tuberosity. Together, they are the primary knee extensors and are essential for all weight-bearing lower-limb function.
1. Rectus Femoris
This is the only quadriceps muscle that crosses both the hip and the knee. It starts at the anterior inferior iliac spine (AIIS) and helps with both hip flexion and knee extension.
Because it crosses both the hip and knee, the rectus femoris is prone to strain during kicking. This happens when hip extension and knee flexion occur at the same time, which is a common injury in football and soccer players.
2. Vastus Lateralis
This is the largest quadriceps muscle. It starts on the side of the femur at the lateral shaft and the linea aspera.
If the lateral quadriceps become much larger than the medial side, this can pull the patella outward. This imbalance can lead to problems with patellar tracking and even cause the patella to partially dislocate to the side.
3. Vastus Medialis
This muscle is on the inner side of the quadriceps. Its lower, slanted fibers, called the vastus medialis oblique (VMO), help balance the outward pull on the patella when the knee straightens.
Problems with the VMO are often linked to patellofemoral pain syndrome. According to the APTA clinical guidelines for PFPS, weakness in the quadriceps, including hip extension, abduction, and external rotation, is common. Strengthening these muscles is supported by good evidence for reducing pain and improving function.
4. Vastus Intermedius
This muscle lies underneath the rectus femoris, between the other vastus muscles. It starts from the front and side of the femur.
The vastus intermedius helps extend the knee. Through its connective tissue, it may also help the articularis genus, a small muscle that pulls the suprapatellar pouch out of the way during knee extension to prevent pinching of the synovial lining.
Posterior Thigh: Hamstrings
The hamstrings are three muscles located at the back of the thigh. Together, they extend the hip and flex the knee. These muscles mainly start from the ischial tuberosity and are the most often strained in sprinting athletes. Injuries usually happen during the last part of the swing phase in running, when the hamstrings slow down rapid knee extension.
1. Biceps Femoris
This muscle has a long head that starts at the ischial tuberosity and a short head that starts at the linea aspera. The long head is supplied by the tibial division of the sciatic nerve, while the short head is supplied by the common fibular nerve.
Biceps femoris flexes the knee and turns the leg outward. Because the short head has a different nerve supply, it can be selectively weakened in common fibular nerve injuries, which is an important clinical clue.
2. Semitendinosus
This is a long, strap-like muscle with a long tendon at its lower end. It helps flex the knee, extend the hip, and rotate the tibia inward.
The tendon is often used as a graft for ACL reconstruction, known as the “hamstring graft,” because it is easy to access, long enough, and has low risk at the donor site.
3. Semimembranosus
This is the deepest and most medial of the hamstring muscles. One of its tendons helps form the oblique popliteal ligament at the back of the knee, which strengthens the back part of the joint capsule.
A bursa sits between the semimembranosus tendon and the inner head of the gastrocnemius muscle. This bursa can connect with the knee joint, and if it fills with fluid, it forms a Baker’s cyst (popliteal cyst), which is often seen by chance on knee MRI.
Inner Thigh: Adductor Group
The adductors move the thigh toward the body’s center and stay active during walking, running, and slowing down sideways. All these muscles start at the pubic rami and ischial tuberosity.
Groin strain, which most often affects the adductor longus, is one of the most common soft tissue injuries in professional soccer, ice hockey, and equestrian sports.
1. Adductor Longus
This is the most forward adductor muscle and the one most often strained. It stretches from the body of the pubis to the middle third of the linea aspera. If there is tenderness where it starts at the pubic bone after sudden groin pain, it is a strong sign of an adductor longus injury.
2. Adductor Brevis
This muscle is shorter and deeper than the adductor longus. It helps bring the thigh inward and also helps with hip flexion. It sits between the front and back branches of the obturator nerve.
3. Adductor Magnus
This is the largest and most complex adductor muscle. It has two parts: the adductor part, which is controlled by the obturator nerve (L2–L4), and the hamstring part, which is controlled by the tibial division of the sciatic nerve (L4–S1).
The hamstring part also helps extend the hip, so the adductor magnus shares some functions with the muscles at the back of the thigh.
The adductor magnus has an opening near its lower end called the adductor hiatus. This is where the femoral artery and vein pass from the front to the back of the thigh and become the popliteal vessels.
4. Gracilis
This is the innermost muscle of the thigh. It is long and flat, running from the lower pubic bone to the inside of the upper tibia, where it joins the pes anserinus.
The gracilis brings the thigh inward, bends the knee, and turns the bent leg inward. Its tendon is the second most commonly used for hamstring grafts in ACL reconstruction, along with the semitendinosus.
Read More – Complete Guide to Thigh Muscle Anatomy: Learn Parts, Names & Diagram
11. Lower Leg Muscles
The lower leg is divided into three main muscle groups: the posterior leg (calf muscles), the anterior leg, and the lateral leg, also known as the fibular (peroneal) group. Each group has a specific role in supporting movement, balance, and stability. In this section, we will explore the anatomy, function, and importance of each of these muscle groups in detail.
Posterior Leg: Calf Group
1. Gastrocnemius
The two-headed gastrocnemius forms the prominent, palpable bulk of the calf. The medial head (larger) and lateral head originate from the posterior femoral condyles and converge distally to join the soleus at the Achilles tendon.
The gastrocnemius crosses both the knee and ankle joints. While its main job is to point the foot downward (plantarflexion), it also helps a little with bending the knee.
Strains of the gastrocnemius, often called “tennis leg,” usually affect the area where the medial head meets the tendon. These injuries often happen suddenly during quick push-off movements, especially in middle-aged recreational athletes.
2. Soleus
The soleus starts at the back of the fibular head, the soleal line of the tibia, and a fibrous arch connecting the two bones. Unlike the gastrocnemius, the soleus only acts at the ankle joint, helping to point the foot downward no matter the knee’s position.
This difference helps clinicians tell the soleus apart from the gastrocnemius during rehab. For example, doing heel raises with bent knees targets the soleus. The soleus is mostly made of slow-twitch muscle fibers, which makes it very resistant to fatigue and good for holding posture.
The soleus is sometimes called the “peripheral heart” because it helps pump blood back to the heart. When you stand or walk, its regular contractions move blood from the deep veins in the calf toward the right atrium.
If the soleus does not work properly, it can increase the risk of deep vein thrombosis (DVT) in people who are not moving much.
Both the gastrocnemius and soleus muscles join together to form the Achilles tendon, which is the thickest and strongest tendon in the body. This tendon attaches to the back of the heel bone.
3. Plantaris
The plantaris is a small, thin muscle with a short muscle belly and a very long tendon. It runs between the gastrocnemius and soleus muscles.
The plantaris does not add much to ankle or knee movement. During surgery, its tendon can sometimes be confused with the sural nerve, and it is sometimes used for tendon grafts.
A tear of the plantaris muscle can cause a snapping sound and pain in the back of the calf. This injury is known but often mistaken for other problems, and it is different from Achilles tendon injuries.
Anterior Leg
1. Tibialis Anterior
The tibialis anterior starts at the lateral tibial condyle and the upper part of the fibula. It is the main muscle that lifts and turns the foot inward. You can see its tendon on the top of the foot when you pull your foot upward.
Weakness or paralysis caused by injury to the common fibular (peroneal) nerve or compression of the L4 nerve root can lead to foot drop. This means the person cannot lift the front of the foot while walking, so they may walk with higher steps at the hip and knee to clear the foot.
2. Extensor Digitorum Longus
The extensor digitorum longus starts at the lateral tibial condyle and the front of the fibula. This muscle straightens the four smaller toes (digits 2 to 5) and helps lift the foot. You can see its four tendons on the top of the foot when you extend your toes.
Lateral Leg: Fibular (Peroneal) Group
1. Fibularis (Peroneus) Longus
The fibularis (peroneus) longus runs behind the lateral malleolus and crosses the sole of the foot from the outside to the inside. It attaches to the base of the first metatarsal and the medial cuneiform.
Because of its diagonal path, the fibularis longus can both point the foot downward and turn it outward, while also supporting the transverse arch. If the fibularis longus tendon slips out of place over the lateral malleolus, often after a sudden forced upward movement of the foot, it can cause a snapping or popping feeling at the ankle.
2. Fibularis (Peroneus) Brevis
The fibularis (peroneus) brevis is shorter and lies deeper than the longus. It starts from the lower part of the fibula and attaches to the styloid process at the base of the fifth metatarsal, which is a common site for avulsion fractures during inversion ankle sprains (“Jones fracture zone”).
The fibularis brevis is the main muscle that turns the foot outward and helps stabilize the outside of the ankle. Strengthening this muscle is important for recovery after a lateral ankle sprain, which is the most common musculoskeletal injury seen in US emergency departments.
FAQ’s
The human body has approximately 600–650 named skeletal muscles. Exact counts vary between anatomical classification systems and whether vestigial or small accessory muscles are included.
The gluteus maximus is the largest by volume and mass. The sartorius (running from the AIIS to the medial tibia) is the longest single muscle. The gluteus medius is often cited as the most biomechanically consequential for healthy gait.
The stapedius muscle of the middle ear, measuring approximately 1 mm in length, is the smallest named skeletal muscle. It dampens the ossicular response to loud sounds, protecting the cochlea.
The deep stabilizers — transversus abdominis, multifidus, and pelvic floor — form the “inner unit” of postural control. The erector spinae, gluteus medius, and rhomboids are the key “outer unit” muscles for maintaining upright alignment of the spine, pelvis, and shoulder girdle.
Foot drop results from weakness or paralysis of the tibialis anterior and extensor group of the anterior compartment, most commonly caused by compression or injury of the common fibular (peroneal) nerve at the fibular head, or by L4 nerve root compression from a lumbar disc herniation.