📅 Published on September 24, 2025 | 🕒 Last Reviewed & Updated on August 1, 2026
- LBP is the single leading cause of disability worldwide — affecting 619 million people (2020), projected 843 million by 2050.[1][2]
- Up to 84% of adults will experience at least one LBP episode during their lifetime; 80% figure widely cited by NIH NINDS.[3][4]
- 90–95% of LBP presentations are nonspecific — no identifiable structural pathology; amenable to conservative care.[4]
- Duration classification: Acute (< 6 weeks) · Sub-acute (6–12 weeks) · Chronic (> 12 weeks). [3]
- Psychosocial factors — depression, anxiety, catastrophizing — are primary drivers of chronification.[5][6]
- Red-flag symptoms including leg weakness, bladder/bowel dysfunction, or unexplained weight loss require urgent evaluation.[4]
Overview of Lower Back Pain Causes
Lower back pain (LBP) is the leading cause of years lived with disability (YLDs) globally, as confirmed by the World Health Organization (WHO).[1]
According to the Global Burden of Disease Study 2021, published in The Lancet Rheumatology, LBP affected 619 million people worldwide in 2020, with projections reaching 843 million by 2050 — a 36% increase driven primarily by population growth and ageing.[2]
Notably, 38.8% of all LBP-related YLDs are attributable to three modifiable factors: occupational exposures, cigarette smoking, and high body mass index.[2]
In the United States, approximately 80% of adults will experience LBP at some point during their lifetime, making it the most common cause of job-related disability and a leading contributor to missed workdays.[3] The lifetime prevalence of back pain may reach 84% when all episodes are included.[4]
The lumbar spine — comprising five vertebrae (L1–L5), intervertebral discs, facet joints, ligaments, and paraspinal musculature — is a complex load-bearing structure supporting nearly every body movement.[4][5]
While LBP often follows a physical trigger such as heavy lifting, twisting, or prolonged sitting, its etiology is frequently multifactorial, integrating structural, biomechanical, and psychosocial components.[4][5]
Clinical Perspective
Age-related spinal degeneration does not inevitably cause pain. Many adults with significant disc degeneration on MRI imaging remain functionally active and pain-free. Pain experience is shaped by biological, psychological, and social factors — the foundation of the biopsychosocial model of pain, endorsed by the 2018 Lancet global LBP series as the current standard of care.[5]
Key Anatomical Structures Involved in Lower Back Pain
Understanding lumbar anatomy contextualizes how and why pain develops. The following structures are most frequently implicated in LBP:
- Intervertebral Discs: Each disc consists of a tough outer annulus fibrosus (composed of approximately 15–20 concentric collagen lamellae) and an inner nucleus pulposus (a proteoglycan-rich, water-retaining gel). The disc is avascular and entirely dependent on nutrient diffusion through vertebral endplate capillaries — a system vulnerable to disruption by ageing, smoking, and sustained mechanical overload.[7]
- Facet Joints: Paired synovial joints at each spinal level that guide and limit motion. Progressive arthritic degeneration of these joints is termed spondylosis and is among the most common sources of chronic LBP.[4]
- Paraspinal Muscles & Ligaments: Provide dynamic spinal stability. The deep stabilisers — particularly the transversus abdominis and multifidus — are critical for segmental control. Acute overload of these structures is the single most common cause of LBP.[4]
- Nerve Roots: Exit the spinal canal through neural foramina at each vertebral level. Compression or chemical irritation produces radicular pain (sciatica) in a dermatomal distribution, with possible motor weakness and sensory deficits.[8]
- Sacroiliac (SI) Joints: Articulate the lumbar spine with the pelvis. SI joint dysfunction can closely mimic lumbar disc pathology in its clinical presentation.[4]
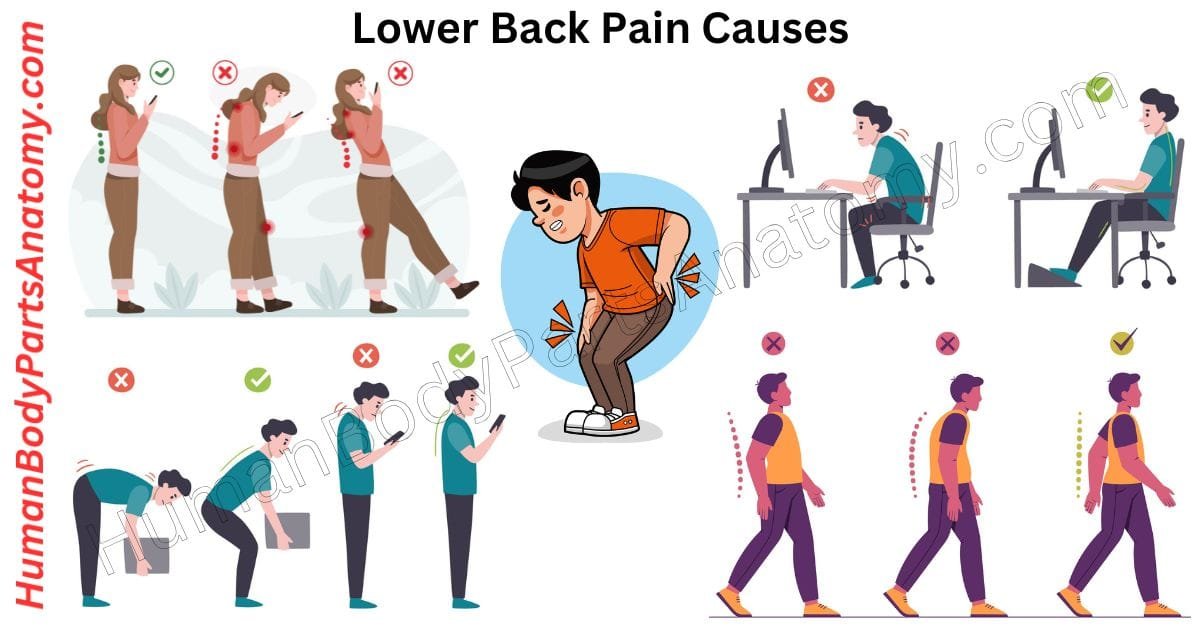
Causes of Lower Back Pain Diagram
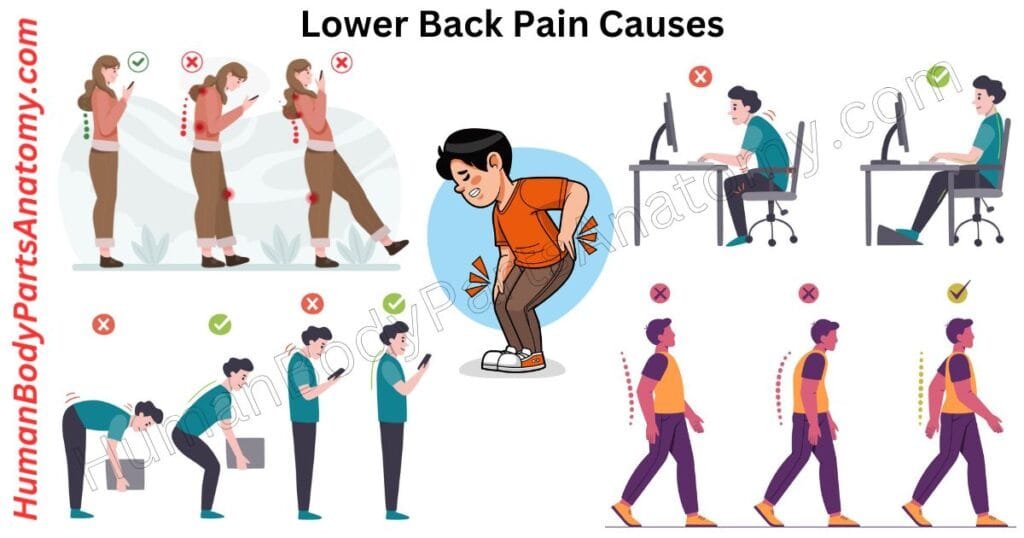
What Causes Lower Back Pain
- Muscle and Ligament Strain (Overuse Injury)
- Intervertebral Disc Injury
- Annular Tear (Disc Tear)
- Herniated Disc (Disc Herniation / Slipped Disc)
- Degenerative Disc Disease (DDD)
- Degenerative Spondylolisthesis
- Spinal Stenosis
- Scoliosis
- Compression Fracture
Lower Back Pain Causes
LBP etiologies are classified as specific (identifiable structural or systemic pathology) or nonspecific (no definitive structural cause identified). Approximately 90–95% of LBP presentations are nonspecific mechanical pain, suitable for conservative management without routine imaging.[4]
Degenerative changes — including disc degeneration, disc bulging, and facet arthropathy — are highly prevalent in asymptomatic adults; imaging findings must be interpreted carefully within the clinical context.
1. Muscle and Ligament Strain (Overuse Injury)
Muscular or ligamentous strain is the most common trigger of acute LBP, especially in younger, active individuals. It occurs when the paraspinal muscles — including the erector spinae, multifidus, and quadratus lumborum — or associated ligaments are subjected to forces beyond their physiological tolerance, resulting in micro-tears, localised inflammation, and protective muscle spasm.[4]
Common triggers: Sudden heavy lifting without adequate preparation, unaccustomed physical activity after a period of inactivity, prolonged static postures (desk work, driving), sports participation, or repetitive axial loading.[3][4]
Pain is characteristically dull, aching, and localised to the lower lumbar region. Most acute episodes resolve within 4–6 weeks with activity modification, analgesics, and progressive mobilisation.[3][4]
2. Intervertebral Disc Injury
The intervertebral discs are among the most commonly injured structures in the lumbar spine, with two principal pathologies:
Annular Tear (Disc Tear)
The annulus fibrosus — the disc’s outer fibrous shell composed of approximately 15–20 collagen lamellae — can develop radial or circumferential fissures through cumulative mechanical stress, sudden compressive loading, or natural ageing. Most annular fissures are asymptomatic; when symptomatic, they produce localised, deep lumbar pain particularly worsened by forward flexion and axial loading.[9]
Inflammatory mediators released at the tear site — including substance P and cytokines — stimulate nociceptors in the outer annular layers and sensitise adjacent nerve fibres, generating discogenic pain even in the absence of frank neural compression. This explains why some patients with annular tears experience severe pain while others remain symptom-free.[9]
Herniated Disc (Disc Herniation / Slipped Disc)
Herniation occurs when the nucleus pulposus protrudes through a deficient or torn annulus fibrosus, potentially impinging upon nerve roots, the dural sac, or, in severe cases, the spinal cord itself.[10]
Approximately 95% of lumbar disc herniations occur at the L4–L5 or L5–S1 levels, compressing the corresponding nerve roots and typically producing classic sciatica: a sharp or burning pain radiating from the lower back through the buttock and down the posterior or lateral leg, accompanied by numbness, tingling (paraesthesia), and potentially focal motor weakness.[8]
Risk factors: Repetitive lumbar flexion-rotation under load, heavy lifting, prolonged sitting, obesity, cigarette smoking, and pre-existing disc degeneration.[10][11]
3. Degenerative Disc Disease (DDD)
Intervertebral discs progressively lose hydration and height with age as the proteoglycan-rich nucleus pulposus desiccates, reducing its shock-absorbing capacity. Advanced disc collapse increases compressive loading on facet joints, producing arthritic friction, stiffness, and reduced range of motion. The resulting facet joint arthrosis — termed spondylosis — can progress to secondary conditions including spinal stenosis and segmental instability.[7][12]
Disc degeneration is detectable on MRI imaging in over 80% of adults older than 50 years, though the presence of degenerative changes alone does not predict pain severity.[4]
Evidence-based preventive strategies:
- Maintaining a healthy body weight to reduce lumbar compressive forces.[13]
- Regular core-stabilising and aerobic exercise to improve disc nutrition through cyclic loading.[4][13]
- Smoking cessation to preserve endplate vascularity and disc cell metabolism.[14]
- Neutral-spine posture and ergonomic workstation corrections to minimise cumulative disc and facet loading.[4][13]
4. Degenerative Spondylolisthesis
Spondylolisthesis refers to the anterior displacement of one vertebral body relative to the one below it. In the degenerative variant, this results from progressive facet joint arthropathy and ligamentous laxity, which compromise segmental stability.[15]
The L4–L5 segment is the most commonly affected level, occurring 6–9 times more frequently than other lumbar levels.[16]
Degenerative spondylolisthesis is uncommon before age 50, but its prevalence rises sharply thereafter, with a significant sex disparity: population data show a prevalence of 8.4% in women versus 2.7% in men — approximately three times higher in women — attributed to age-related hormonal changes that reduce ligamentous tensile strength.[15]
Vertebral slippage may compress exiting nerve roots or narrow the central canal, producing back pain, neurogenic claudication (leg pain worsened by walking or standing, relieved by sitting), and in severe cases, bowel or bladder dysfunction.[15]
5. Spinal Stenosis
Spinal stenosis is the pathological narrowing of the spinal canal, compressing the spinal cord or exiting nerve roots.[13]
It is most prevalent after age 50 and is strongly associated with age-related degenerative changes: intervertebral disc height loss, facet joint hypertrophy, and thickening of the ligamentum flavum. A minority of patients are born with a congenitally narrow canal, predisposing them to stenotic symptoms at a younger age. Additional risk factors include obesity and a positive family history. [17]
6. Scoliosis
Scoliosis is an abnormal lateral curvature of the spine, forming an “S” or “C” shape instead of a straight vertical alignment. It most commonly develops during adolescent growth spurts (adolescent idiopathic scoliosis), though adults — particularly those with pre-existing osteoarthritis — can develop degenerative scoliosis. When progressive or severe, scoliosis causes chronic LBP and, if nerve roots are compressed by the deformity, lower extremity weakness or radicular pain. Early detection enables timely intervention to prevent curve progression.[4]
7. Vertebral Compression Fracture
Vertebral compression fractures (VCFs) occur when one or more vertebral bodies crack or collapse under compressive force. Osteoporosis — characterised by reduced bone mineral density and microarchitectural deterioration of bone tissue — is the most common underlying cause. VCFs are the most common osteoporotic fracture, with an estimated 700,000 occurring annually in the United States.[18]
Additional causes include high-energy trauma (motor vehicle accidents, falls from height), pathological fractures secondary to bone metastases or primary bone malignancies such as multiple myeloma, and prolonged corticosteroid therapy.[4][18]
Multiple adjacent VCFs produce progressive anterior vertebral wedging, resulting in kyphosis — the forward thoracolumbar curvature clinically recognised as a “dowager’s hump”.[19]
Signs & Symptoms of Lower Back Pain
LBP encompasses a broad symptom spectrum — from a dull, persistent ache to sharp, electric, or burning pain — and may radiate into the buttock, thigh, calf, or foot depending on its underlying cause. It significantly limits mobility and impairs occupational performance, sleep, and psychosocial well-being. [1][3]
Types of Low Back Pain
- Acute LBP (< 6 weeks): Most episodes are self-limiting and resolve with conservative care.[3]
- Sub-acute LBP (6–12 weeks): Warrants structured management to prevent progression to chronicity.[3]
- Chronic LBP (> 12 weeks): Requires a multidisciplinary, biopsychosocial approach. Approximately 20% of patients with acute LBP develop chronic LBP with persistent symptoms at one year.[3][5]
Common Symptoms
- Pain Quality: Dull and aching (muscular or discogenic); sharp or stabbing (facet joint); electric, burning, or shooting (neuropathic or radicular).[4]
- Pain Onset: Abrupt (muscle strain, fracture) or insidious (degeneration, stenosis, malignancy).[4]
- Radiation Pattern: Localised to the lumbosacral region, or radiating into the buttock, posterior thigh, calf, or foot — classic sciatica or radiculopathy following a dermatomal distribution.[8]
- Morning Stiffness: Most pronounced after sleep or prolonged inactivity; typically improves with gentle movement — characteristic of degenerative or inflammatory origins.[4]
- Postural Disturbance: Antalgic lean (lateral trunk shift), loss of lumbar lordosis, or difficulty achieving and maintaining an upright stance.[4]
- Muscle Spasm: Involuntary, painful tightening of paraspinal muscles as a protective response to underlying tissue injury; may limit movement significantly.[4]
Radicular Symptoms (Sciatica)
Sciatic nerve compression — most commonly from disc herniation or foraminal stenosis at L4–L5 or L5–S1 — produces a characteristic syndrome of unilateral lower-extremity pain, paraesthesia (tingling or numbness), and potential motor deficit. True sciatica follows a specific dermatomal distribution, distinguishing it from referred somatic pain, which tends to be more diffuse and poorly localised. At L4–L5, pain radiates into the lateral leg and dorsum of the foot; at L5–S1, pain radiates into the posterior calf and plantar surface.[8]
Impact on Daily Functioning
Chronic LBP extends well beyond physical symptoms. Research demonstrates strong associations between persistent LBP and depression, anxiety, sleep disturbance, cognitive impairment, and reduced social participation. In occupational settings, chronic LBP is a leading cause of presenteeism, long-term work absence, and premature retirement — a substantial socioeconomic burden. [1][5]
Red Flag Symptoms: When to Seek Immediate Medical Attention
The following symptoms — individually or in combination — may indicate a serious underlying pathology (cauda equina syndrome, cord compression, spinal infection, malignancy, or fracture) and require immediate clinical evaluation.[4]
- Bladder or bowel incontinence or retention — possible cauda equina syndrome; a surgical emergency requiring urgent decompression.[4]
- Progressive bilateral leg weakness or saddle anaesthesia (perineal numbness).[4]
- Severe, unrelenting pain not relieved by any position — particularly nocturnal pain.[4]
- Unexplained significant weight loss (> 4.5 kg / 10 lbs over 6 months without intent).[4]
- Known or suspected malignancy with new-onset back pain.[4]
- Recent significant trauma (motor vehicle accident, fall from height, contact sport injury).[4]
- Fever, rigors, or recent invasive spinal procedure — raises concern for spinal epidural abscess or infective discitis.[4]
- Age > 70 with new-onset back pain — substantially elevated risk of osteoporotic fracture and occult malignancy.[4][18]
Risk Factors for Lower Back Pain
Biological, behavioural, and environmental factors substantially elevate the risk of developing LBP or experiencing recurrence. Modifiable risk factors are also actionable targets for prevention. [4][5]
Non-Modifiable Risk Factors
- Age: The incidence and severity of LBP rise progressively from the third decade of life, peaking around ages 40–60 years. Disc degeneration is detectable on MRI in over 80% of adults older than 50 years, though degeneration alone does not predict clinical pain.[4]
- Biological Sex: Women experience a higher lifetime LBP prevalence than men, particularly in association with pregnancy, postmenopausal osteoporosis, and hormonal changes affecting connective tissue laxity. The peak number of LBP cases occurs at age 50–55 years.[1][4]
- Genetic Predisposition: Twin studies demonstrate that the heritability of lumbar disc degeneration reaches up to 74% (assessed by MRI lumbar disc degeneration score). [6] For LBP pain specifically, heritability estimates from the Finnish Twin Cohort range from 30–46%. [6] Conditions such as scoliosis and spondylolisthesis also demonstrate familial clustering. A prior history of LBP is the single strongest predictor of future episodes.[4]
Modifiable Risk Factors
- Physical Inactivity and Deconditioning: Weak core musculature — particularly the transversus abdominis and lumbar multifidus — reduces spinal segmental stability and increases compressive loads on discs and facet joints. Regular core-stabilising exercise is among the most evidence-supported prevention strategies.[4][5]
- Obesity and Excess Body Weight: Abdominal obesity increases lumbar compressive forces, accelerates intervertebral disc degeneration, promotes systemic low-grade inflammation, and is independently associated with chronic LBP. Occupational factors, smoking, and high BMI together account for 38.8% of all LBP-related disability globally.[2][4]
- Occupational Hazards: Heavy manual labour, repetitive lifting and bending, prolonged sedentary work, and whole-body vibration (common among heavy vehicle operators) are well-established occupational LBP risk factors. Occupational exposures are the largest single attributable risk factor for LBP-related YLDs.[2][4]
- Poor Ergonomics: Non-ergonomic workstation setup, prolonged unsupported sitting, and poor postural habits during sustained computer use contribute to cumulative paraspinal fatigue and spinal loading.[4][13]
- Cigarette Smoking: Nicotine causes vasoconstriction of the microvasculature surrounding intervertebral discs, impairing oxygen and nutrient delivery through vertebral endplate capillaries. Nicotine also down-regulates chondrocyte proliferation and glycosaminoglycan (GAG) biosynthesis in disc cells, accelerating degeneration. Smoking additionally promotes chronic cough, which repeatedly elevates intradiscal pressure.[14]
- Psychosocial Factors: Depression, anxiety, pain catastrophising, fear-avoidance beliefs, and workplace dissatisfaction are among the strongest predictors of LBP chronification and poor treatment outcomes — in many studies, more predictive than structural imaging findings. The 2018 Lancet LBP series identifies these factors as central to modern management.[5][6]
- Improper Lifting Mechanics: Lumbar flexion-rotation under load substantially increases intradiscal pressure and annular stress. Training in neutral-spine lifting technique is a cornerstone of occupational injury prevention programmes.[4]
Prevention Strategies: Protecting Your Lumbar Spine
The following strategies are supported by current evidence for reducing the incidence, recurrence, and severity of LBP. [4][5][13]
- Core Strengthening: Progressive exercise targeting the deep stabilisers (transversus abdominis, multifidus) and global movers (erector spinae, gluteals) provides essential dynamic spinal support and significantly reduces recurrence rates.[4][13]
- Regular Aerobic Exercise: Walking, swimming, cycling, and low-impact aerobics maintain spinal mobility, improve disc nutrition through cyclic loading, and reduce central sensitisation associated with chronic pain.[4][13]
- Weight Management: Even modest weight reduction (5–10% of body weight) meaningfully reduces lumbar compressive forces, improves disc health, and reduces systemic inflammatory burden.[4][13]
- Smoking Cessation: Cessation restores disc endplate vascularity and disc cell metabolism, reducing both the biological and behavioural contributors to LBP.[14]
- Ergonomic Optimisation: Adjustable lumbar-support seating, eye-level monitor positioning, sit-stand workstations, and scheduled microbreaks significantly reduce cumulative spinal strain in desk-based workers.[4][13]
- Mental Health & Stress Management: Mindfulness-based stress reduction (MBSR), cognitive behavioural therapy (CBT), and adequate sleep have demonstrated efficacy in reducing LBP risk and improving chronic pain outcomes.[5][6]
Conclusion
Lower back pain is a complex, multidimensional condition spanning a spectrum from self-limiting musculoligamentous strain to progressive neurological compromise. While most episodes resolve with conservative care, a thorough understanding of anatomy, pathophysiology, and clinical presentation is essential for accurate diagnosis, effective treatment, and meaningful prevention.
The 2018 Lancet global LBP series — now the international clinical benchmark — recognises that psychosocial contributors, lifestyle factors, and central sensitisation mechanisms are integral to both the onset and persistence of LBP.[5] The biopsychosocial model is no longer supplementary; it is foundational. Long-term spinal health requires a holistic strategy — not merely episodic pain management.
If you or a patient are experiencing persistent or worsening lower back pain, early consultation with a qualified spine specialist, physical therapist, or primary care physician remains the most effective first step toward recovery.[4]
FAQ’s
Lumbar muscle and ligament strain — from overuse, sudden activity, or improper lifting — is the most frequent cause. In clinical settings, disc herniation, degenerative disc disease, and lumbar spondylosis are the most common structural diagnoses.[4]
Yes. Psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis, elevates cortisol, and triggers sustained paraspinal muscle tension. The biopsychosocial model recognises emotional and cognitive factors as primary drivers of pain experience and chronification — not merely secondary contributors.[5][6]
Intervertebral discs act as fibrocartilaginous shock absorbers between vertebral bodies. When they degenerate, herniate, or develop annular tears, they can chemically sensitise or mechanically compress adjacent neural structures, producing local or radicular pain.[7][8][9]
The facet joints, intervertebral joints, and sacroiliac joints are often involved. Degeneration, inflammation, or misalignment in these joints can contribute to discomfort.
Red-flag symptoms requiring urgent medical evaluation include: rapidly worsening pain; leg numbness or weakness; difficulty walking; fever; unexplained weight loss; or changes in bladder or bowel function. These may indicate cauda equina syndrome, spinal infection, or malignancy.[4][18]
There is a meaningful genetic component. Twin studies show heritability of lumbar disc degeneration reaching up to 74% on MRI scoring. For LBP pain itself, heritability estimates range from 30–46% in the Finnish Twin Cohort. Family history is a clinically relevant risk factor.[6]
Yes. Constipation can cause lower back pain when backed-up stool increases pressure on the lower spine and surrounding nerves, leading to discomfort or aching. Pain may improve once bowel movements become regular, but persistent symptoms should be evaluated by a healthcare provider.
Yes. Uterine fibroids—noncancerous growths in the uterus—can cause lower back pain if they grow large enough to press on pelvic nerves or nearby structures. This pain may feel dull, aching, or persistent and is often associated with heavy menstrual bleeding or pelvic pressure.
Lower back pain just above the buttocks is commonly caused by muscle strain, poor posture, sacroiliac (SI) joint dysfunction, or lumbar disc issues. It may also result from overuse, prolonged sitting, or underlying spinal conditions that affect the lower lumbar region.
Lower back pain is most often caused by muscle strain, poor posture, repetitive movements, or age-related spinal changes such as disc degeneration. In some cases, it may signal nerve compression, arthritis, kidney problems, or other medical conditions—especially if pain is severe, persistent, or accompanied by numbness or fever.
References-
- World Health Organization. Low Back Pain — Key Facts. Reviewed June 2023.
URL: WHO Low Back Pain Fact Sheet - GBD 2021 Low Back Pain Collaborators. (2023). Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021.
PMID: 37271545 | PMCID: PMC10234592 | DOI: 10.1016/S2665-9913(23)00098-X
URL: PubMed Reference - National Institute of Neurological Disorders and Stroke (NINDS/NIH). Low Back Pain Fact Sheet. Last reviewed 2022.
URL: NINDS Low Back Pain Fact Sheet - Casiano VE, Sarwan G, Dydyk AM, Varacallo MA. (2025). Back Pain.
NCBI Bookshelf ID: NBK538173
URL: NCBI Bookshelf Reference - Foster NE, Anema JR, Cherkin D, et al. (2018). Prevention and treatment of low back pain: evidence, challenges, and promising directions.
PMID: 29573872 | DOI: 10.1016/S0140-6736(18)30489-6
URL: PubMed Reference - Sambrook PN, MacGregor AJ, Spector TD. (1999). Genetic influences on cervical and lumbar disc degeneration: a magnetic resonance imaging study in twins.
PMID: 10025932
URL: PubMed Reference - Waxenbaum JA, Reddy V, Williams C, Futterman B. (2025). Anatomy, Back, Intervertebral Discs.
NCBI Bookshelf ID: NBK470583
URL: NCBI Bookshelf Reference - Al Qaraghli MI, De Jesus O. (2023). Lumbar Disc Herniation.
NCBI Bookshelf ID: NBK560878
URL: NCBI Bookshelf Reference - Tenny S, Gillis CC. (2023). Annular Disc Tear.
NCBI Bookshelf ID: NBK459235
URL: NCBI Bookshelf Reference - Dydyk AM, Ngnitewe Massa R, Mesfin FB. (2025). Disk Herniation.
NCBI Bookshelf ID: NBK441822
URL: NCBI Bookshelf Reference - Dydyk AM, Varacallo MA. (2023). Lumbar Degenerative Disk Disease.
NCBI Bookshelf ID: NBK448134
URL: NCBI Bookshelf Reference - Dydyk AM, Ngnitewe Massa R, Mesfin FB. (2023). Lumbosacral Disc Injuries.
NCBI Bookshelf ID: NBK448072
URL: NCBI Bookshelf Reference - National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS/NIH). Back Pain — Overview, Diagnosis, Treatment, and Steps to Take. Last reviewed 2023.
URL: NIAMS Back Pain Overview - Rajesh N, Milner A, Vo N, Sheridan D, Elliott D. (2022). Smoking and degenerative spinal disease: A systematic review. Brain and Spine, 2, 100916.
PMCID: PMC9560562 | DOI: 10.1016/j.bas.2022.100916
URL: PMC Full Article - Tenny S, Gillis CC. (2025). Spondylolisthesis.
NCBI Bookshelf ID: NBK430767
URL: NCBI Bookshelf Reference - Kalichman L, Hunter DJ. (2008). Diagnosis and conservative management of degenerative lumbar spondylolisthesis. European Spine Journal, 17(3), 327–335.
PMID: 18026865 | PMCID: PMC2270383 | DOI: 10.1007/s00586-007-0543-3
URL: PubMed Reference - Munakomi S, Cruz R. (2024). Lumbar Spinal Stenosis.
NCBI Bookshelf ID: NBK531493
URL: NCBI Bookshelf Reference - LeBoff MS, Greenspan SL, Insogna KL, et al. (2022). New Osteoporotic/Vertebral Compression Fractures.
NCBI Bookshelf ID: NBK279035
URL: NCBI Bookshelf Reference - Becker BA, Childress MA. (2025). Vertebral Compression Fractures.
NCBI Bookshelf ID: NBK448171
URL: NCBI Bookshelf Reference
Medical Disclaimer
All content on HumanBodyPartsAnatomy.com is educational and based on verified, peer-reviewed medical sources. Articles are authored or reviewed by qualified medical or biomedical professionals to ensure accuracy.
This website does not provide medical advice, diagnosis, or treatment. Always consult a licensed healthcare professional for personal medical guidance.
No commercial or promotional interests influence the medical content published on this site.