📅 Published on January 10, 2024 | 🕒 Last Reviewed & Updated on July 17, 2026
Overview of Nail Anatomy
Nails are flat, protective structures found at the tips of the fingers and toes and are a defining feature of most primates. [2] They are composed of keratin — a tough, flexible protein that also constitutes hair and the outer skin layer, which enables nails to grow continuously and withstand daily mechanical stress. [1] Nails protect sensitive fingertip tissues, enhance grip and precision, and contribute to tactile sensation. [1] Every nail is unique in shape, texture, and growth rate, reflecting individual genetic and physiological differences. [2]
The nail anatomy is both complex and well-organised. Each nail consists of several distinct structures, including the hard nail plate, the vascularised nail bed, and the nail matrix, which drives nail growth. [1] The lunula — a pale, half-moon shape near the base — represents the visible portion of the matrix. [1] The cuticle seals the proximal nail fold and protects the matrix from infection. [3]
This article explores each anatomical component in detail, explaining its structure and function to help you understand how nails grow, protect, and support everyday hand and foot health.
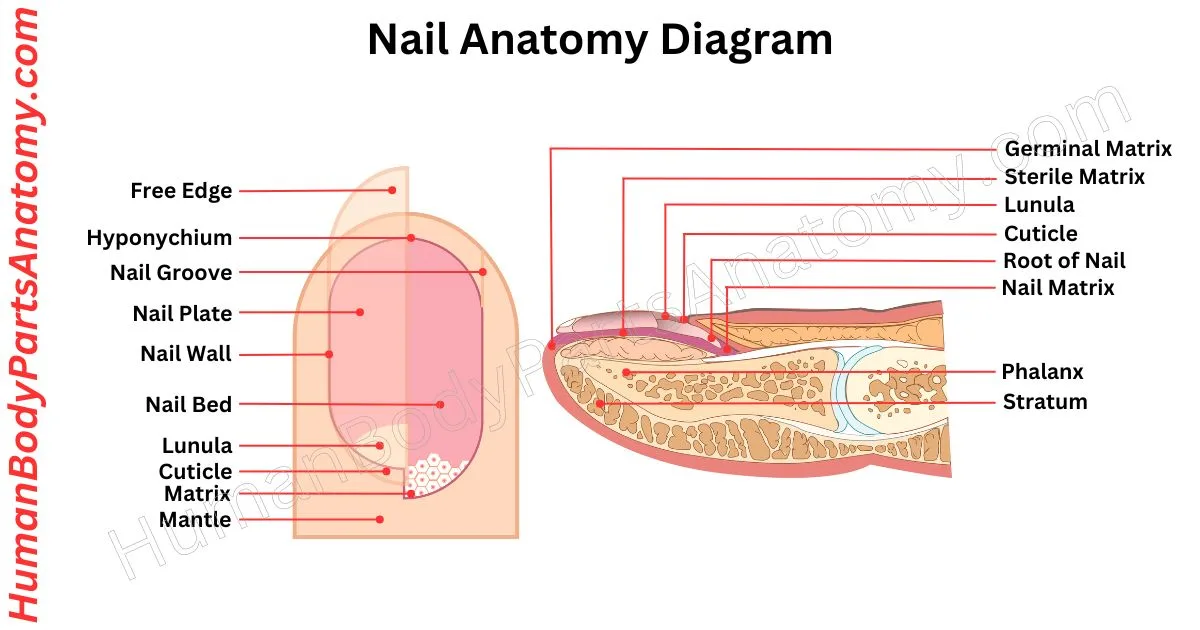
Nail Anatomy Diagram
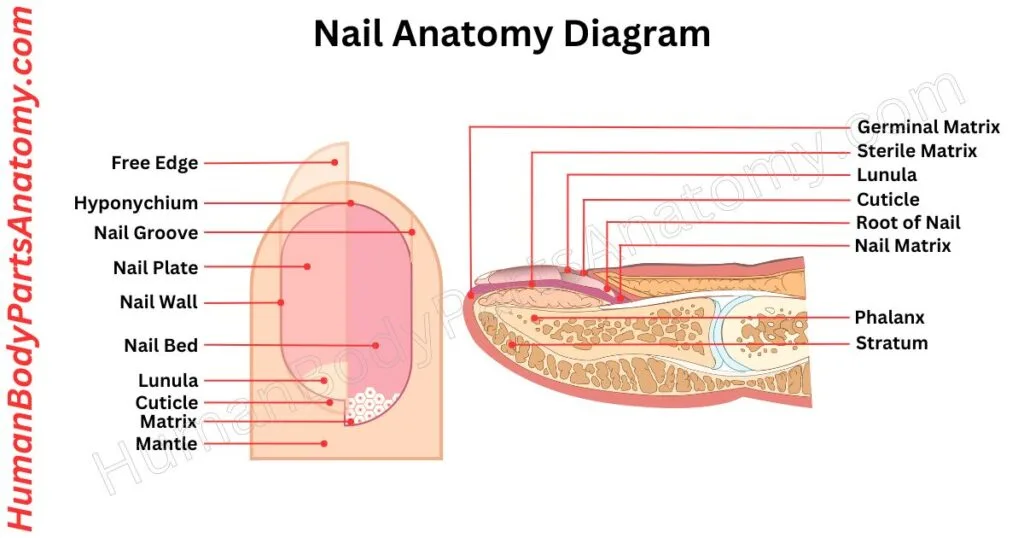
Parts of the Nail
- Nail Plate
- Nail Bed
- Nail Bed Blood Supply
- Matrix
- Lunula
- Cuticle
- Nail Folds
- Nail Grooves
- Nail Root
- Eponychium
- Hyponychium
- Nail Horn
- Nail Nerves
- Nail Bed Arteries and Veins
Nail Anatomy: Parts & Functions
Nail Plate
The nail plate is the hard, keratinised structure that covers and protects the fingertip and is the most visible part of the nail unit.[1] It is composed of approximately 196 rows of compact, well-differentiated keratinocytes called onychocytes.
The plate is translucent because fully mature nail cells lose their nuclei during keratinisation, allowing light to pass through to the pink nail bed beneath.[2]
The nail plate attaches to the nail bed through complementary longitudinal epidermal ridges that interlock to maximise adhesion, ensuring the free edge can function as a tool without loosening the plate or causing pain.[1]
It is acceptable to lightly buff the plate surface during nail treatments; however, aggressive filing or repeated layer removal can weaken the structure, resulting in a thin and sensitive nail.[1]
Nail Bed
The nail bed is the soft tissue attached to the underside of the nail plate. It begins distal to the lunula and terminates at the hyponychium, and contains a rich network of blood vessels that nourish the fingertip.[1]
The nail plate is anchored to the nail bed through longitudinal epidermal ridges — complementary structures on both surfaces that increase attachment area and enhance adhesion.[1]
Through the continuous production of new nail cells — a process called onychogenesis — the nail matrix constantly supplies fresh onychocytes that are pushed distally to form and extend the nail plate.[1]
Nail Bed Blood Supply
The nail bed is served by a dense network of capillaries arranged in ridges that run parallel to the direction of nail growth.[1]
Arterial blood is supplied by the superficial palmar arch via the common and proper digital arteries, which branch proximal to the distal interphalangeal joint into dorsal and palmar digital vessels.[1]
Extensive anastomoses (arterial connections) between these vessels ensure continued blood flow even when the fingers grip tightly.[1]
When the fingers perform active tasks, blood flow to the nail bed increases to meet the metabolic demands of the matrix.[1]
When exposed to cold temperatures, the sympathetic nervous system triggers the release of norepinephrine, which acts on alpha-adrenergic receptors to cause vasoconstriction of the digital arteries and cutaneous arterioles, reducing peripheral blood flow and conserving core body temperature.[5]
Matrix
The nail matrix is the specialised generative tissue located beneath the proximal nail fold. The proximal portion of the matrix begins approximately halfway between the distal interphalangeal joint and the proximal nail fold.
The distal portion of the matrix is visible through the translucent nail plate as the white half-moon structure called the lunula.[1]
The matrix is the only component of the nail unit that contains melanocytes — pigment-producing cells. It also harbours Langerhans cells and Merkel cells.[1]
As the nail grows, onychocytes are pushed superficially and distally from the matrix. Approximately 80% of the nail plate is produced by the proximal nail matrix, while the distal matrix contributes the remainder.[1]
This is why biopsies or surgery limited to the distal matrix produce minimal lasting damage to the nail plate.[1]
Lunula
The lunula is the white, crescent-shaped structure visible at the base of the proximal nail. It represents the distal portion of the nail matrix visible through the transparent nail plate.[1]
The matrix appears white in this region because the thickened epidermis and the light-scattering effect of nucleated living cells prevent light from reaching the pink vascular nail bed beneath. As cells mature, flatten, and lose their nuclei, this opacity disappears, and the plate becomes transparent.[1]
The size and prominence of the lunula are primarily determined by genetics rather than general health status.[2]
However, changes in lunula morphology — including colour shifts, loss of definition, or abnormal enlargement — can serve as clinical indicators of systemic conditions such as anaemia, thyroid disease, and connective tissue disorders.[9]
Cuticle
The cuticle is a thin, transparent layer of cornified (dead) stratum corneum that grows over the nail plate at the proximal nail fold, forming a continuous protective seal between skin and nail.[3]
Together with the proximal nail fold, the cuticle shields the nail matrix from environmental pathogens, moisture, and irritants.[1]
Because the cuticle is non-living tissue, it may be carefully trimmed or gently pushed back to improve nail product adhesion and appearance.
However, aggressive or repeated removal disrupts the protective seal, increasing the risk of infection and matrix damage.[1]
Nail Folds
Nail folds are soft tissue structures that protect the proximal and lateral edges of the nail plate.[1] The proximal nail fold covers most of the nail matrix, shielding it from mechanical trauma and ultraviolet radiation.[1]
The lateral nail folds extend along both sides of the nail, providing lateral structural support and directing the nail plate to grow correctly in the longitudinal axis.[6]
Nail Groove
Nail grooves run on either side of the nail plate, framing it and providing the anatomical anchor point for the lateral nail folds.[3]
Without the structural coupling of the groove and fold, the nail plate would be susceptible to dislodging, lifting, and detachment during normal activity.[1]
The depth and configuration of the nail groove vary between individuals based on genetic factors, nutritional status, and overall health.[1]
Nail Root
The nail root — functionally equivalent to the nail matrix — is situated deep within the skin beneath the proximal nail fold.
It is the generative centre responsible for producing the cells that form the visible nail plate.[1] Complete replacement of a fingernail after loss requires approximately 100–180 days (3–6 months); toenail regrowth typically takes 12–18 months.[6]
Any condition that disrupts the matrix’s regenerative capacity — systemic illness, nutritional deficiency, or trauma — leaves a structural record in the outgrowing nail plate (for example, Beau’s lines or thinning), much as climatic changes are recorded in tree growth rings.[9]
Eponychium
The eponychium is the living skin at the visible lip of the proximal nail fold. It is frequently confused with the cuticle: the cuticle is the non-living cornified layer shed onto the nail plate surface, while the eponychium is the living dermal tissue that generates the cuticle and forms the final seal of the protective barrier.[1]
Because the eponychium is living tissue, it must not be cut. Keeping it hydrated and gently retracted preserves its integrity.
Regular emollient application supports the periungual skin and protects the barrier function of the eponychium without causing damage.[1]
Hyponychium
The hyponychium is the specialised epithelium beneath the free edge of the nail plate, occupying the zone where the nail plate and nail bed begin to separate.[1]
Histologically, it is characterised by a thick stratum granulosum, strong keratinisation, and the presence of basal melanocytes. It forms a sealed barrier that prevents external debris and pathogens from penetrating the subungual space.[4]
Aggressive cleaning beneath the free nail edge with pointed instruments injures the hyponychium, causing pain, bleeding, and breach of the seal. This can trigger onycholysis — separation of the nail plate from the nail bed — predisposing the nail to bacterial and fungal infection.[1]
Nail Horn
The nail horn is the portion of the nail plate that extends beyond the fingertip as a continuously growing, tightly packed layer of dead keratinised cells.[2]
Although insensitive to pain (it contains no nerve endings), the free edge plays an important functional role: it provides rigid counter-pressure behind the fingertip pulp, amplifying tactile discrimination and enabling fine motor tasks such as typing, playing musical instruments, and reading braille.[1]
Nail Nerves
The nail unit is richly innervated by branches of the proper digital nerves, which travel along both sides of each digit. Dorsal branches cross the distal interphalangeal joint to supply the skin near the nail folds; palmar branches run alongside the digital arteries and subdivide to cover the nail bed and fingertip pulp.[1]
This dense innervation underpins the exceptional tactile discriminative capacity of the human fingertip.[1]
Nail Bed Arteries & Veins
The nail bed is served by a rich arteriovenous system whose primary function is delivering oxygen and nutrients to the nail bed and matrix. Anastomotic channels ensure perfusion is maintained during high-pressure gripping.[1]
Disruption of this vascular network — through infection, inflammation, or systemic disease — produces characteristic nail changes such as splinter haemorrhages, which can serve as clinical indicators of both local and systemic pathology.[9]
The nail unit consists of the nail plate (hard keratinised outer layer), nail bed (vascularised skin beneath the plate), nail matrix (generative tissue), lunula (visible white crescent of the matrix), cuticle (cornified protective layer at the proximal fold), and hyponychium (sealed epithelium beneath the free edge).[1]
Nails grow from the matrix, where keratinocytes divide and undergo keratinisation. Fingernails grow at an average of approximately 3.47 mm per month, while toenails grow at approximately 1.62 mm per month.[7] Growth rate varies with age, nutrition, season, circulation, and systemic health.
The nail matrix produces onychocytes that determine the nail’s shape, thickness, and growth rate. The proximal matrix generates approximately 80% of the nail plate. Damage — from trauma, surgery, or infection — can cause permanent ridging, thinning, or deformity.[1]
The lunula is the white half-moon at the nail base — the distalmost visible segment of the nail matrix seen through the translucent plate. It appears white because living nucleated cells scatter light before it reaches the vascular dermis below. Its size is genetically determined. Changes in lunula appearance can be associated with systemic conditions such as anaemia and thyroid disorders.[9]
White spots on nails, termed leukonychia, most commonly result from minor trauma to the nail matrix causing a localised disruption of normal keratinisation. No robust scientific evidence links white spots to calcium deficiency. Leukonychia typically resolves as the nail grows out. Persistent, widespread, or patterned leukonychia warrants medical evaluation to exclude systemic disease, drug reactions, or fungal infection.[8]
Key measures include: keeping nails clean and dry; trimming straight across; avoiding nail biting or picking; applying emollient to periungual skin; and consuming a balanced diet adequate in protein, biotin, zinc, and iron. Avoid aggressive sub-ungual cleaning and excessive buffing. Persistent nail changes should prompt consultation with a healthcare provider or dermatologist.[1]
References-
- Johnson C, Sinkler MA, Schmieder GJ. StatPearls [Internet] — NIH / NLM NCBI Bookshelf. (2023). Anatomy, Shoulder and Upper Limb, Nails. https://www.ncbi.nlm.nih.gov/books/NBK534769/ Last Update: June 5, 2023. Treasure Island (FL): StatPearls Publishing.
- Brahs AB, Bolla SR. StatPearls [Internet] — NIH / NLM NCBI Bookshelf. (2023). Histology, Nail. https://www.ncbi.nlm.nih.gov/books/NBK539733/ Last Update: May 29, 2023. PMID: 30969555. Treasure Island (FL): StatPearls Publishing.
- Institute for Quality and Efficiency in Health Care (IQWiG). InformedHealth.org — NIH / NLM NCBI Bookshelf. (2024). In brief: Structure of the nails. https://www.ncbi.nlm.nih.gov/books/NBK513133/ Reviewed: July 29, 2024.
- Eshaghi MA et al. StatPearls [Internet] — NIH / NLM NCBI Bookshelf. (2024). Onychoscopy. https://www.ncbi.nlm.nih.gov/books/NBK585099/ Last Update: October 6, 2024. Treasure Island (FL): StatPearls Publishing.
- Browning J, Bhatt DL, Hackshaw KV. StatPearls [Internet] — NIH / NLM NCBI Bookshelf. (2023). Raynaud Disease. https://www.ncbi.nlm.nih.gov/books/NBK499833/ Last Update: August 8, 2023.
- Alston MA et al. StatPearls [Internet] — NIH / NLM NCBI Bookshelf. (2023). Anatomy, Bony Pelvis and Lower Limb: Toe Nails. https://www.ncbi.nlm.nih.gov/books/NBK544338/ Last Update: August 14, 2023.
- Yaemsiri S, Hou N, Slining MM, He K. Journal of the European Academy of Dermatology and Venereology. (2010). Growth rate of human fingernails and toenails in healthy American young adults. JEADV. 24(4):420–423. https://pubmed.ncbi.nlm.nih.gov/19744178/ PMID: 19744178. DOI: 10.1111/j.1468-3083.2009.03426.x.
- Iorizzo M, Starace M, Pasch MC. American Journal of Clinical Dermatology (Springer Nature). (2022). Leukonychia: What Can White Nails Tell Us? Am J Clin Dermatol. 23(2):177–193. https://pmc.ncbi.nlm.nih.gov/articles/PMC8809498/ PMID: 35112320. PMC: PMC8809498. DOI: 10.1007/s40257-022-00671-6.
- Singal A, Arora R. Indian Dermatology Online Journal — NIH / PMC. (2015). Nail as a window of systemic diseases. Indian Dermatol Online J. 6(2):67–74. https://pmc.ncbi.nlm.nih.gov/articles/PMC4375768/ PMID: 25821724. PMC: PMC4375768. DOI: 10.4103/2229-5178.153002.
Read More-
Human Body-
- Human Anatomy: Guide to Bones, Muscles, Organs, Systems, Functions & Diagram
- Human Skeleton Anatomy: All 206 Bones Explained with Functions & Diagrams
- Human Muscle Anatomy: Validated Guide to Every Major Muscles & Functions
Head, Face & Senses-
- Nose Anatomy: Parts of the Nose, Structure, Nasal Cavity & Sinuses Explained
- Skull Anatomy: Parts of the Skull, Structure, Cranial, Facial Bones & Functions
- Mouth Anatomy: Guide on Parts of Mouth, Lips, Palate, Gums & Oral Cavity
- Eye Anatomy: Parts of the Eye, Cornea, Lens, Retina, Optic Nerve & Diagram
- Ear Anatomy: Parts of the Ear, Outer, Middle & Inner Ear & Structures
Brain & Nervous System-
- Brain Anatomy: Parts of the Brain, Structure, Functions & Regions Explained
- The 4 Lobes of the Brain: Complete Guide with Locations & Functions
Spine & Back-
- Cervical Spine Anatomy: C1–C7 Vertebrae, Muscles & Nerves Explained
- Spine Anatomy: Parts of the Spine, Vertebrae, Curves, Spinal Cord & Diagram
- Neck Muscle Anatomy: Guide with Key Muscles, Groups, Functions & Diagrams
- Rib Cage Anatomy: Ribs, Sternum, Thoracic, Vertebrae & Functions Explained
Organs-
- Pancreas Anatomy: Parts of Pancreas, Structure, Location, Functions & Role
- Stomach Anatomy: Parts of Stomach, Regions, Layers & Digestive Function
- Heart Anatomy: Guide on Parts of Heart, Chambers, Valves & Blood Flow
- Liver Anatomy: Key Parts of Liver, Functions, Lobes, Segments & Diagram
- Kidney Anatomy: Guide on Parts of Kidney, Structure, Functions & Diagram
Upper Limb-
- Forearm Anatomy: Parts of the Forearm, Radius, Ulna, Muscles & Diagram
- Shoulder Anatomy: Parts of the Shoulder, Bones, Joint Structure & Diagram
- Wrist Anatomy: Parts of the Wrist, 8 Carpal Bones, Tendons & Diagram
- Hand Anatomy: Parts of the Hand, Bones, Muscles with Functions & Diagram
- Finger Anatomy: Parts of Finger, Bones, Joints, Muscles, Tendons & Diagram
- Biceps Brachii Anatomy: Parts of Bicep, Structure, Functions & Diagram
- Arm Anatomy: Parts of Arm, Bones, Muscles & Joints with Functions & Diagram
Lower Limb-
- Hip Muscle Anatomy: Guide on Key Muscle Groups, Names, Functions & Diagram
- Hip Bone Anatomy: Parts of Hip Bone, Ilium, Pubis, Functions & Diagram
- Femur Anatomy: Parts of Femur, Structure, Functions, Location & Diagram
- Leg Anatomy: Parts of the Leg, Bones, Muscles & Lower Leg with Functions
- Knee Anatomy: Parts of Knee, Bones, Ligaments, Cartilage & Joint Structure
- Thigh Muscle Anatomy: Key Muscle Groups, Names, Functions & Diagram
Medical Disclaimer
All content on HumanBodyPartsAnatomy.com is educational and based on verified, peer-reviewed medical sources. Articles are authored or reviewed by qualified medical or biomedical professionals to ensure accuracy.
This website does not provide medical advice, diagnosis, or treatment. Always consult a licensed healthcare professional for personal medical guidance.
No commercial or promotional interests influence the medical content published on this site.
Medical Disclaimer
All content on HumanBodyPartsAnatomy.com is educational and based on verified, peer-reviewed medical sources. Articles are authored or reviewed by qualified medical or biomedical professionals to ensure accuracy.
This website does not provide medical advice, diagnosis, or treatment. Always consult a licensed healthcare professional for personal medical guidance.
No commercial or promotional interests influence the medical content published on this site.