📅 Published on June 9, 2024 | 🕒 Last updated on July 4, 2026
Overview of Femur Anatomy
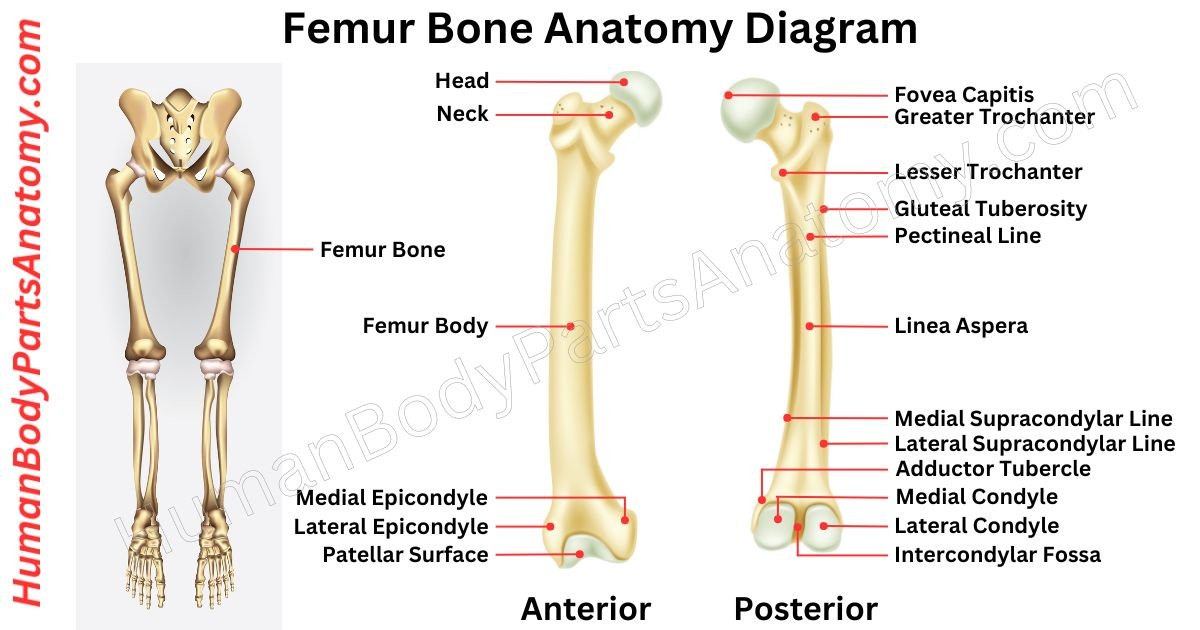
The femur, or thigh bone, is the main bone in your thigh.[1] It connects your hip to your knee and is your body’s largest and strongest bone.[1][2] In animals with four legs, it is the upper bone in the back leg. The femur anatomy has several parts: the shaft, head, neck, and more.[1] The top part fits into your hip joint, and the bottom connects to your shinbone (tibia) and kneecap (patella) to form your knee.[1] Humans have two femurs, one in each leg, and they meet at the knees, connecting to the tibiae. The angle where they meet affects the angle of your knees.[1] The femur is about 26.74% of a person’s height, so it can help estimate the height of someone from their skeleton.[1][3]
This article will show the detailed femur bone anatomy with its parts, names, functions & diagrams. It will help us to understand more about the human body parts.
Femur Anatomy Diagram
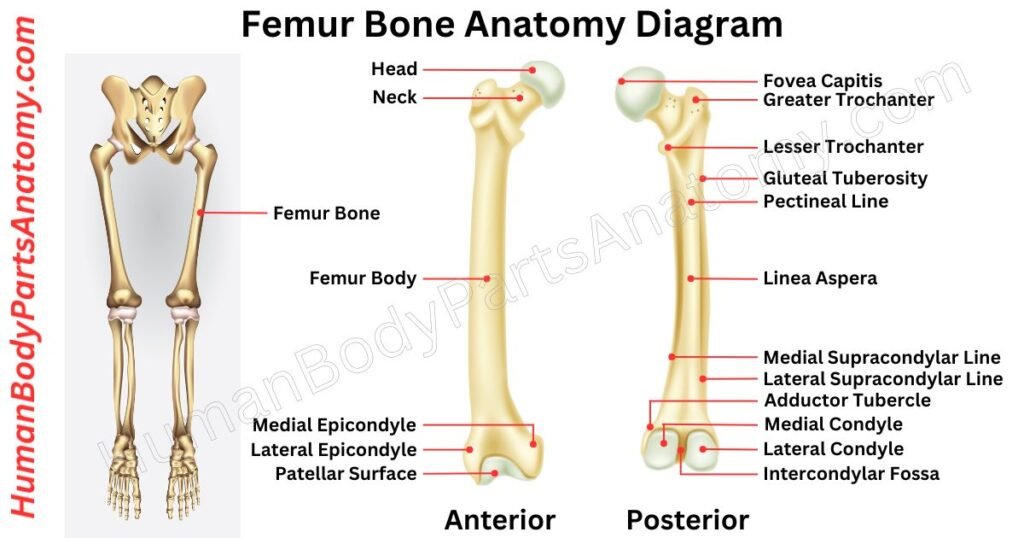
Parts of Femur
- Femoral Head
- Femoral Neck
- Femur Shaft
- Greater Trochanter
- Lesser Trochanter
- Medial & Lateral Condyles
- Intercondylar Notch
- Epicondyles
- Patellar Groove
- Linea Aspera
- Medial Supracondylar Ridge
- Lateral Supracondylar Ridge
- Medial Femoral Intermuscular Septum
- Lateral Femoral Intermuscular Septum
- Gluteal Tuberosity
- Adductor Tubercle
- Femoral Shaft Angles
- Nutrient Foramen
- Medullary Cavity
Femur Anatomy
Femoral Head
The femoral head is the rounded top part of the thigh bone (femur).[1] It connects to the femoral neck and fits into the acetabulum of the pelvis, forming the hip joint.[1][2]
The femoral head is shaped like a ball.[1] It has a small pit called the fovea capitis femoris, where a ligament attaches.[2] This area is important because it can suffer from avascular necrosis, especially after hip injuries.[2]
The femoral head acts as the “ball” in the hip joint, allowing a wide range of motion. It is covered with smooth cartilage, which helps it move easily against the acetabulum.[1]
Inside the femoral head, there are different patterns of trabeculae (small, beam-like structures within the bone):
- Primary Compressive Group: These trabeculae run vertically from the top of the femoral head to the inner neck, bearing the main load.[2][4]
- Primary Tensile Group: These run from the bottom of the femoral head to the outer side of the femur, handling tensile (stretching) forces.[2][4]
- Secondary Compressive Group: These follow additional stress lines within the upper femur.[2][4]
- Secondary Tensile Group: These align with tensile forces in the outer upper femur.[2][4]
- Greater Trochanteric Group: These follow stress lines within the greater trochanter, a bony prominence on the femur.[2][4]
There is an area with fewer trabeculae called Ward’s triangle, which is a weak spot in the bone. It differs from Babcock’s triangle, a region seen on X-rays where hip tuberculosis often occurs.[2]
Femoral Neck
The femoral neck is a connecting bone structure between the femoral head and shaft. It is shaped like a flattened pyramid, with a wider angle outward.[1]
The neck is flat from front to back, narrower in the middle, and wider on the outer side compared to the inner side.[1]
The lateral half of the neck has a larger vertical diameter due to its sloping lower edge. It joins the body near the lesser trochanter. This side measures about one-third more than its front-to-back diameter. The medial half is smaller and more circular.[1]
The front of the neck has many small holes for blood vessels. There are slight grooves along the top front where the hip joint capsule fibers sit.[1]
The back of the neck is smooth, broader, and more concave than the front. The hip joint capsule attaches about 1 cm above the intertrochanteric crest.[1]
The top border is short and thick. It ends at the greater trochanter and has large holes for vessels. The bottom border is longer and narrower. It curves slightly backward to reach the lesser trochanter.[1]
Femur Shaft
The femur, or your thigh bone, angles slightly inward and brings your knees closer to your body center to maintain balance.[1]
On the backside of the femur, there are rough ridges called the rough line or linea aspera. These ridges split below into two lines, medial and lateral supracondylar lines, with a flat area(the popliteal surface) in between.[1]
Near the top, the rough line becomes the pectineal line on the inside and the rough gluteal tuberosity outside, where your gluteus maximus muscle attaches.[1]
Towards the bottom, the linea aspera widens and becomes part of the popliteal fossa. The medial and lateral borders become the medial and lateral supracondylar lines.[1]
The medial supracondylar line ends at the adductor tubercle, where the adductor magnus muscle attaches.[1]
Greater Trochanter
The greater trochanter of the femur is a major, bony projection on the side of the thigh bone. It extends outward and slightly backward from the hip joint.[1]
In adults, it typically sits 2–4 cm below the top of the femur. However, in females, due to a wider pelvic outlet than males, there is a greater in-between distance of the greater trochanters.[1]
On its outer side, the greater trochanter is broad and rough. It is shaped like a quadrilateral. It has a diagonal groove where the tendon of the gluteus medius muscle attaches.[1]
This attachment occurs with areas above and below this groove that may be roughened or smooth with a cushioning bursa.[1]
On the inner side, there is a smaller, deep vale known as the trochanteric fossa, where the tendon of the obturator externus muscle attaches.[1]
Lesser Trochanter
In human anatomy, the lesser trochanter is a small, cone-shaped bump inside the femur (thigh bone). It is located where the shaft of the femur meets the neck of the femur, towards the back and slightly below.[1]
The main function of the lesser trochanter is to serve as the attachment point for the iliopsoas muscle, which is important for hip movement.[1]
The top and front surfaces of the lesser trochanter are rough, while the back surface is smooth.[1] From its highest point, three distinct borders extend:
- A medial border that continues with the lower edge of the femoral neck.[1]
- A lateral border that merges with the intertrochanteric crest.[1]
- An inferior border that blends with the middle section of the linea aspera, a ridge on the femur.[1]
Medial & Lateral Condyle
The lower end of the femur has two projections: the medial and lateral condyles. The medial condyle is bigger because it bears more weight since the body’s center leans toward the inner side of the knee.[1]
On the back of the medial condyle, a ridge splits into two parts: the medial and lateral supracondylar ridges.[1]
The most distant ridge on the inner side of the medial condyle is called the “medial epicondyle,” which you can feel by running your fingers from the patella inward when the knee is bent. The extra part of the medial femoral condyle helps the knee rotate passively.[1]
The lateral condyle is the other ridge on the femur’s lower end. It is more prominent and wider from front to back and side to side compared to the medial condyle.[1]
Intercondylar Fossa/ Notch
The intercondylar fossa of the femur is like a deep groove between two bumps at the bottom of your thigh bone. These bumps are called the medial and lateral epicondyles.[1]
They are the parts that connect to your knee. The bumps are smoother and not pronounced on the front side of your thigh bone. There is a flat area called the patellar surface where your kneecap fits.[1]
You might also hear these areas called the patellar groove, patellar sulcus, or trochlear groove of the femur. They are all different ways of talking about the same parts of your knee joint.[1]
Epicondyle
The medial epicondyle of the femur is a bony protrusion on the inner side of the thigh bone’s lower end. It is above the medial condyle and has a bump called the adductor tubercle.[1]
It is the portion where muscles attach. This bump separates the thigh muscles into groups. Behind it, there is a rough area where a calf muscle attaches. The lateral epicondyle is smaller and less noticeable.[1]
It connects to a ligament in the knee. Below it is a groove that curves upward and backward on the back end of the bone.[1]
Patellar Surface & Groove
The patellar surface of the femur is a groove-like area at the lower front part of the thigh bone. This groove is between the inner and outer parts of the lower femur.[1]
It connects with a ridge on the patella (kneecap), forming the patellofemoral joint. This joint allows the kneecap to smoothly slide over the end of the thigh bone when we bend or straighten our knee.[1]
Linea Aspera
The linea aspera is a prominent bony ridge located on the posterior side of the femur or thigh bone. This structure is an attachment site for various muscles and connective tissues, effectively dividing the thigh into three distinct compartments.[1]
The linea aspera features two primary edges, the medial and lateral lips, with a roughened area in between.
It provides critical attachment points for the adductor muscles that move the leg toward the body’s midline.[1]
The intermuscular septa are connective tissues that separate different groups of thigh muscles. The distinctive ridges of the linea aspera are formed by the mechanical pull of the attached muscles, gradually shaping the bone over time.[1]
Medial Supracondylar Ridge
The medial supracondylar line is a ridge on the back of the femur. It runs down from the inner part of the thigh bone. It is not as clear as its counterpart on the outside of the bone.[1]
This line starts at the top of the back of the femur and goes down to the adductor tubercle. It divides the back of the thigh bone into the popliteal area and the inner part.[1]
For muscles, this line is where the vastus medialis muscle starts from and where the adductor magnus muscle attaches to.[1]
Lateral Supracondylar Ridge
The lateral supracondylar line is a ridge on the back of the femur. It is part of the bone that runs along the outer edge of the thigh bone.[1]
This line is a mark where certain leg muscles start. These muscles are the plantaris muscle and part of the biceps femoris muscle. It helps separate different areas of the femur bone and plays a role in muscle attachment.[1]
Medial Femoral Intermuscular Septum
The medial femoral intermuscular septum is a thick sheet of tissue that divides the muscles in your thigh. It sits between the thigh’s front and inner (adductor) parts. It stretches from the outer fascia to a ridge on your thigh bone called the linea aspera.[1]
Lateral Femoral Intermuscular Septum
The lateral femoral intermuscular septum is a tough layer of deep fascia that runs between the thigh muscles. It divides the front and back compartments of the thigh.[1]
The lateral femoral intermuscular septum starts from the outer fascia (fascia lata). It attaches along the linea aspera of the femur shaft. It stretches to the hip crest above and the outer knee bone below.[1]
Gluteal Tuberosity
The gluteal tuberosity is a part of the femur bone where the gluteus maximus muscle attaches. It is one of three bony ridges that extend upwards from the back of the femur and start from the linea aspera.[1]
This tuberosity can either appear as a long dent or a rough bump. It runs vertically from the linea aspera up to the base of the greater trochanter, another bony part of the femur.[1]
Adductor Tubercle
The adductor tubercle is a typical bony prominence found at the top of the inner bulge of the thigh bone’s knobby part.[1]
It marks the end of the upper line on the inner side of the thigh bone. It is the portion where the lowest part of the adductor magnus muscle attaches.[1]
The adductor tubercle is located in front and below the prominent point on the inner bulge of the thigh bone, known as the medial epicondyle. This area is where the ligament that connects the thigh bone to the shin bone is anchored.[1]
Femoral Shaft Angles
In the femur anatomy, the angle between the femoral neck and shaft (neck-shaft angle, NSA) varies among people and ancient humans. In adults today, it typically ranges from 120 to 140 degrees. Some have angles less than 120 degrees (coxa varus), while others exceed 140 degrees (coxa valgus).[1]
Nutrient Foramen
The nutrient foramen on the femur shaft is the primary entry point for the nutrient artery into the marrow cavity. Knowledge of its precise location is crucial in surgery and fracture assessment to ensure fractures do not intersect these vital openings.[1]
FAQ’s-
The femur, also called the thigh bone, is the longest and strongest bone in the human body. It is located in the upper leg and connects the hip joint to the knee joint. The femur supports body weight and plays a critical role in walking, running, and jumping. It also helps maintain balance and posture.[1][2]
The femur has three main parts: the proximal end (including the head, neck, greater trochanter, and lesser trochanter), the long shaft in the middle, and the distal end (with condyles and epicondyles for knee articulation).[1]
The femur supports body weight, enables leg movement, and transfers forces between the hip and knee joints. It also provides attachment points for major muscles involved in posture, balance, and locomotion.
The femur is extremely dense and structurally designed to withstand high loads from standing, walking, and running. Its thick cortical bone and cylindrical shape allow it to resist bending, compression, and torsional forces better than any other bone.[1]
Yes, the femur is widely recognized as the strongest bone in the human body.[1][2] Research shows it can withstand compression forces of approximately 800–1,100 kilograms (1,760–2,425 pounds) depending on age, bone density, and health.[5][6] This strength is essential for maintaining mobility and supporting body weight.[1]
The average adult femur measures about 18 inches (45–50 cm) in length, though this varies based on height, sex, and ethnicity.[1] The femur typically accounts for about one-quarter of a person’s total height.[3][1] It is the longest bone in the skeletal system and plays a key role in stature and mobility.[1]
The femur is the largest bone in the human body in terms of length, mass, and strength.[1][2] It forms the upper leg and connects the hip to the knee. The femur supports body weight, enables movement, and withstands the highest mechanical loads in the skeleton.[1]
References-
- National Center for Biotechnology Information. (2023). Anatomy, Bony Pelvis and Lower Limb: Femur. StatPearls Publishing.
PMID: 30422577. Last reviewed: November 17, 2023.
https://www.ncbi.nlm.nih.gov/books/NBK532982/ - National Center for Biotechnology Information. (2023). Anatomy, Bony Pelvis and Lower Limb: Fovea Capitis Femoris. StatPearls Publishing.
PMID: 30335248. Last reviewed: August 8, 2023.
https://www.ncbi.nlm.nih.gov/books/NBK519005/ - Trotter, M., & Gleser, G. C. (1992). Femur/stature ratio and estimates of stature in children. American Journal of Physical Anthropology.
PMID: 1580352.
https://pubmed.ncbi.nlm.nih.gov/1580352/ - Li, X., et al. (2025). Functional morphology of trabecular system in human proximal femur: A perspective from P45 sectional plastination and 3D reconstruction finite element analysis. Bone Research.
PMCID: PMC11993998. Published: April 12, 2025.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11993998/ - Zhang, Q., et al. (2022). The biomechanical behavior of 3D printed human femoral bones under compressive loads. Journal of Orthopaedic Research, 40(12), 2845–2856.
PMCID: PMC9685985 — PMID: 36373714.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9685985/ - O’Brien, F. J. (2018). Bone mechanical properties in healthy and diseased states. National Library of Medicine (PMC).
PMCID: PMC6053074.
https://pmc.ncbi.nlm.nih.gov/articles/PMC6053074/
Read More-
Lower Limb
- Complete Guide on Leg Anatomy with Parts, Functions & Diagram
- Complete Guide to Thigh Muscle Anatomy: Learn Parts, Names & Diagram
- Knee Anatomy: Complete Guide to Parts, Names, Functions & Diagram
Upper Limb
- Complete Guide to Finger Anatomy with Parts, Names, Functions & Diagram
- Comprehensive Guide to Arm Anatomy: Parts, Names & Diagram
- Comprehensive Guide to Hand Anatomy: Parts, Functions & Diagram
- Ultimate Guide to Bicep Anatomy: Parts, Names, Functions & Diagram
- Shoulder Anatomy: Ultimate Guide to Parts, Names, Functions & Diagram
- Wrist Anatomy: Ultimate Guide to Parts, Names, Functions & Diagram
- Complete Guide to Nail Anatomy with all Parts, Names & Diagrams
Official websites of the United States government
- What is Femur Shaft Fracture (Broken Thighbone) & their Types?
- How to do Femur fracture repair?
- All you need to know about Femur X-Ray.
Medical Disclaimer
All content on HumanBodyPartsAnatomy.com is educational and based on verified, peer-reviewed medical sources. Articles are authored or reviewed by qualified medical or biomedical professionals to ensure accuracy.
This website does not provide medical advice, diagnosis, or treatment. Always consult a licensed healthcare professional for personal medical guidance.
No commercial or promotional interests influence the medical content published on this site.