📅 Published on April 7, 2024 | 🕒 Last updated on May 20, 2026
Overview of Shoulder Anatomy
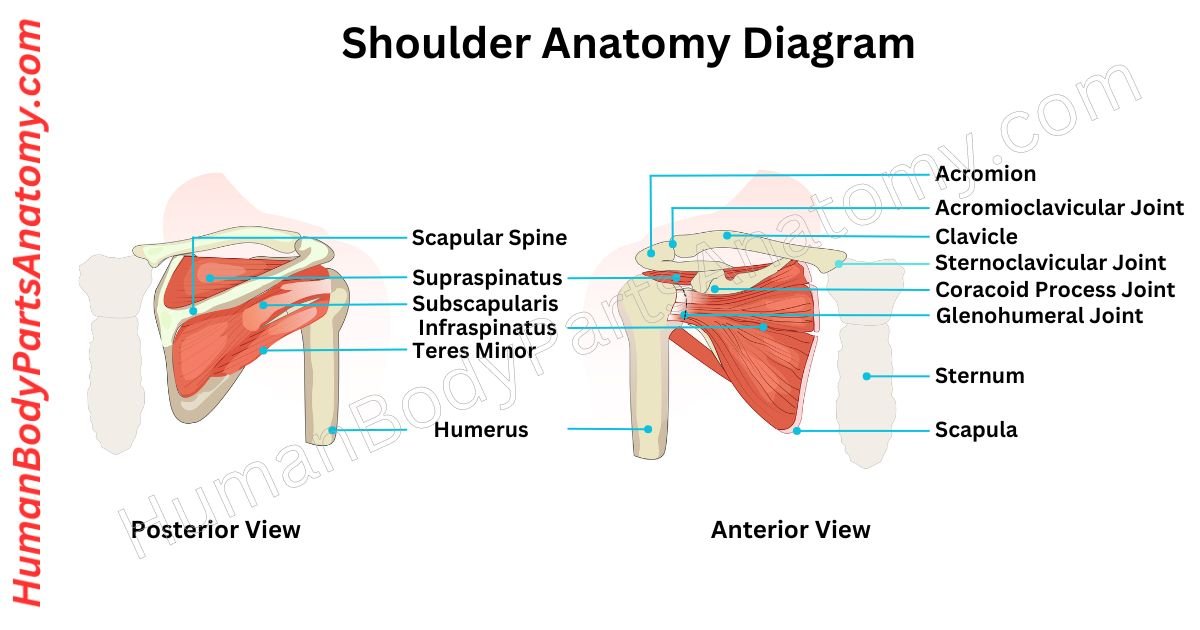
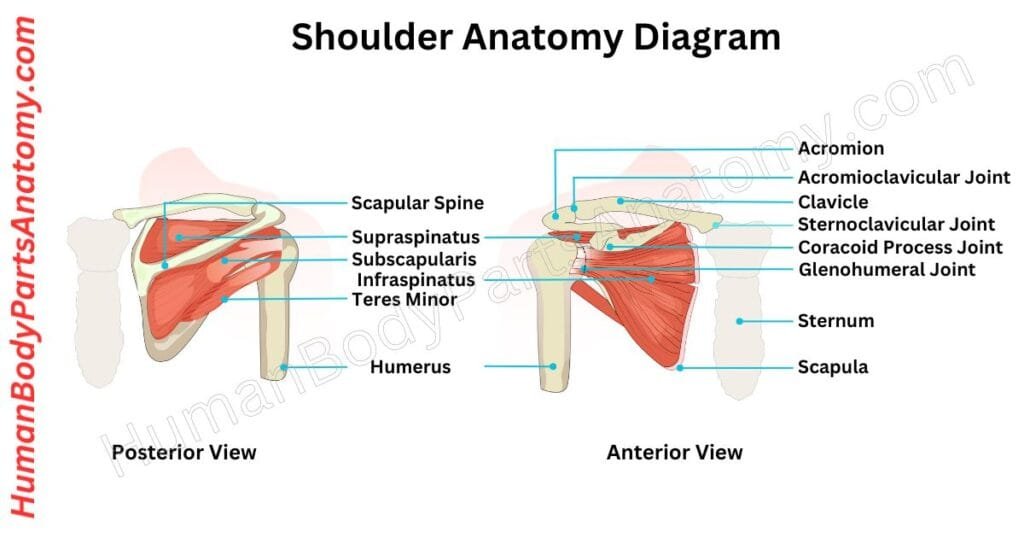
The human shoulder anatomy is composed of three bones: the clavicle (collarbone), scapula (shoulder blade), and humerus (upper arm bone).[1][2] These bones are connected by joints, with the primary articulation being the glenohumeral joint, commonly referred to as the shoulder joint.[2] Additional joints, including the acromioclavicular (AC) joint, the sternoclavicular (SC) joint, and the scapulothoracic articulation, are integral to the complete shoulder complex.[2][3] The glenohumeral joint enables circular rotation and lifting of the arm away from the body.[3] It functions as a ball-and-socket articulation in which the rounded head of the humerus rests within the shallow glenoid cavity of the scapula.[3] A fibrous sleeve called the joint capsule surrounds the glenohumeral joint; its inner surface is lined by a smooth synovial membrane that secretes synovial fluid to reduce friction during movement.[4]
A group of four muscles, collectively called the rotator cuff, maintains shoulder stability.[2][5] These muscles originate on the scapula and insert onto the proximal humerus. They are the supraspinatus, subscapularis, infraspinatus, and teres minor.[5]
Shoulder Anatomy Diagram
Parts of a Shoulder
Bones
- Scapula (Shoulder Blade)
- Clavicle (Collarbone)
- Humerus (Upper Arm Bone)
Joints
- Glenohumeral Joint
- Acromioclavicular Joint
- Sternoclavicular Joint
Muscles
- Deltoid
- Rotator Cuff Muscles
- Biceps Brachii
- Triceps Brachii
Ligaments
- Glenohumeral Ligaments
- Coracohumeral Ligament
- Transverse Humeral Ligament
- Coracoacromial Ligament
Tendons
- Rotator Cuff Tendons
- Biceps Tendon
- Deltoid Tendon
- Long Head of Triceps Tendon
Bursae
- Subacromial
- Subscapular
Shoulder Anatomy Bones
Scapula (Shoulder Blade)
The scapula, or shoulder blade, is a flat, triangular bone situated on the posterior (dorsal) surface of the thorax, overlying ribs two through seven.[6]
Together with the clavicle and the manubrium of the sternum, it forms the shoulder (pectoral) girdle, linking the upper limb to the axial skeleton.[6]
The scapula is of particular importance because approximately 17 different muscles attach to it, making fractures relatively uncommon despite its exposed position.[6]
It articulates with both the humerus (forming the glenohumeral joint) and the clavicle (forming the acromioclavicular joint).[6]
Because the medial border of the scapula is not directly fixed to the axial skeleton but is held in place entirely by muscles, the scapula is free to glide across the posterior thoracic wall at the scapulothoracic articulation.[6]
This mobility provides the upper limb with a substantially greater functional range of motion compared with the lower extremity.[4]
Clavicle (Collarbone)
The clavicle is a sigmoid (S-shaped) long bone that runs horizontally across the anterior superior chest, serving as the primary bony connection between the sternum and the shoulder blade.[7]
It is the only bone positioned horizontally in the human body and is subcutaneous along its entire length, making it readily palpable.[7]
The clavicle acts as a strut, maintaining the arm’s distance from the thorax and enabling an unimpeded range of shoulder motion.[7]
It also disperses and redirects forces transmitted from the upper limb to the axial skeleton, protecting underlying neurovascular structures including the brachial plexus and subclavian vessels.[7]
Humerus (Upper Arm Bone)
The humerus is the largest bone of the upper arm. It is conventionally described in three regions: the proximal end, the shaft, and the distal end.[8]
Prominent landmarks include the humeral head, anatomical neck, greater and lesser tubercles, intertubercular (bicipital) groove, surgical neck, deltoid tuberosity, radial (spiral) groove, and the medial and lateral epicondyles distally.[8]
At its proximal end, the spherical humeral head articulates with the glenoid cavity of the scapula, forming the glenohumeral joint and permitting multiaxial shoulder movement.[8]
At its distal end, the trochlea and capitulum articulate with the ulna and radius respectively, forming the elbow joint.[8]
The elbow’s unique pivot joint configuration allows forearm supination (palm-up rotation) and pronation (palm-down rotation), motions not replicated elsewhere in the body.[9]
Shoulder Anatomy Joints
Glenohumeral Joint/ Shoulder Joint
The glenohumeral joint is the principal articulation of the shoulder, connecting the upper arm to the body.[3] Structurally it is a ball-and-socket joint and functionally a diarthrodial, multiaxial joint—the most mobile joint in the human body.[3]
The humeral head is substantially larger than the shallow glenoid cavity, creating a wide range of motion at the inherent cost of bony stability.[3][4]
Because the joint relies primarily on the rotator cuff muscles, ligaments, glenoid labrum, and joint capsule for stability rather than on bony congruence, it is the most frequently dislocated joint in the body, accounting for up to 45% of all dislocations.[3]
Acromioclavicular Joint
The AC joint is formed where the lateral end of the clavicle meets the acromion process of the scapula.[2] It is an essential joint for shoulder function, particularly for overhead arm elevation.[4]
Unlike the glenohumeral joint, no muscles act directly upon it; accordingly, its movements are passive, resulting from forces transmitted through the adjacent shoulder girdle.[10]
The AC joint permits three planes of motion: protraction–retraction (forward–backward), elevation–depression (upward–downward), and axial rotation.[10]
Its primary functional role is to enable coordinated scapular movement once the sternoclavicular joint has reached its range limit, and to transmit forces from the arm to the clavicle.[10]
Sternoclavicular Joint
The sternoclavicular joint, a saddle-shaped synovial joint, is the only direct skeletal articulation between the upper limb and the axial skeleton.[10][11]
It connects the medial end of the clavicle to the manubrium of the sternum and the superior surface of the first costal cartilage.[11]
The SC joint permits three main motion planes: elevation–depression, protraction–retraction, and axial rotation. These coordinated movements allow the upper limb to move freely in concert with the thorax.[11]
Several critical vascular and neural structures lie immediately posterior to the SC joint, including the brachiocephalic arterial trunk, internal jugular vein, and common carotid artery, as well as the vagus nerve, phrenic nerve, trachea, and esophagus.[11]
In addition to its role in upper-limb mechanics, the SC joint and its bony components protect these vital mediastinal structures.[11]
Shoulder Anatomy Muscles
Deltoid
The deltoid is a powerful, triangular muscle that drapes over the glenohumeral joint. It originates from the clavicle, acromion, and spine of the scapula, and inserts on the deltoid tuberosity of the humerus.[5]
The deltoid comprises three functional portions: the anterior (clavicular) part, which flexes and medially rotates the arm; the middle (acromial) part, which abducts the arm; and the posterior (scapular spinal) part, which extends and laterally rotates the arm.[5]
Together, these three portions enable multi-directional arm movement while providing dynamic stabilisation during overhead and loaded activities.[5]
Rotator Cuff Muscle
The rotator cuff is a group of four muscles and their associated tendons that collectively stabilise the glenohumeral joint and enable shoulder rotation.[2][5] The four rotator cuff muscles are the supraspinatus, infraspinatus, teres minor, and subscapularis.[5]
Each originates from the scapula and inserts onto the greater or lesser tubercle of the humerus, with their tendons blending into the joint capsule to form a continuous stabilising cuff.[5]
The rotator cuff maintains the humeral head centered within the glenoid cavity during all arm movements, and together with the deltoid, generates the force couples required for normal shoulder biomechanics.[5]
Rotator cuff pathology is the leading cause of shoulder pain in the United States, with shoulder pain affecting approximately 18 million Americans annually, the majority of cases attributable to rotator cuff tears.[2]
Biceps Brachii
The biceps brachii is a two-headed muscle of the anterior upper arm that crosses both the shoulder and elbow joints.[9]
Its long head originates from the supraglenoid tubercle of the scapula and its short head from the coracoid process of the scapula. Both heads unite and insert on the radial tuberosity of the forearm.[9]
The primary actions of the biceps brachii are flexion of the forearm at the elbow (forearm flexion) and forearm supination (turning the palm upward). This muscle is critical for activities involving lifting and carrying loads.[9]
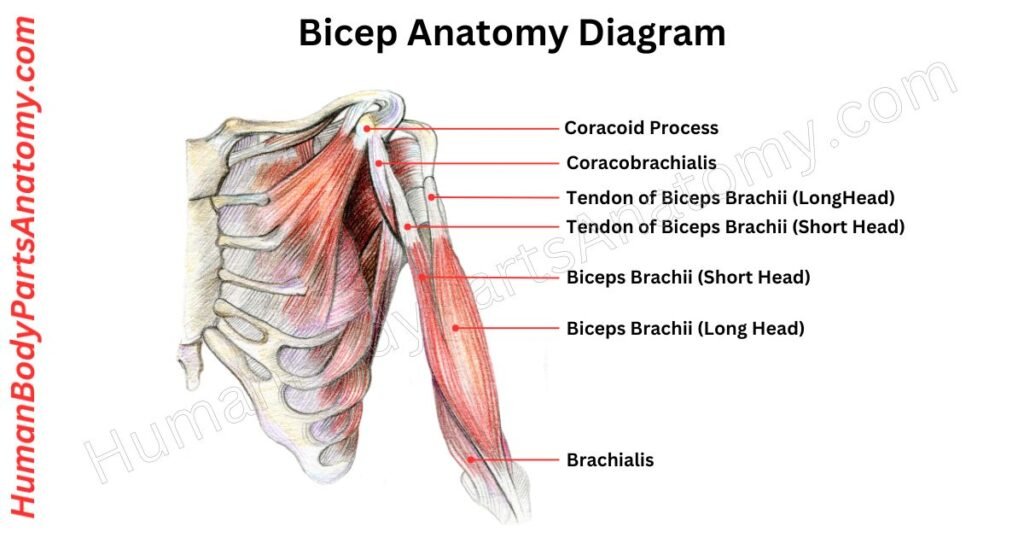
Read More – Ultimate Guide to Bicep Anatomy: Parts, Names, Functions & Diagram
Triceps Brachii
The triceps brachii is the principal extensor of the forearm at the elbow. It is a three-headed muscle: the long head originates from the infraglenoid tubercle of the scapula, while the lateral and medial heads originate from the posterior surface of the humerus. All three heads converge to insert on the olecranon of the ulna.[15]
The triceps brachii extends the elbow during pushing and pressing activities. In addition, the long head contributes to adduction and extension of the arm at the glenohumeral joint. [15]
Shoulder Anatomy Ligaments
Glenohumeral Ligament
The shoulder capsule is reinforced by three distinct glenohumeral ligaments: the superior, middle, and inferior glenohumeral ligaments.[4]
These ligaments extend from the margin of the glenoid fossa to the anatomical neck of the humerus, reinforcing the anterior and inferior aspects of the joint capsule.[4]
Their primary function is to resist anterior and inferior displacement of the humeral head, thereby preventing glenohumeral dislocation.[4]
Coracoclavicular Ligament
The coracoclavicular ligament is a robust band that reinforces the acromioclavicular joint by connecting the coracoid process of the scapula to the inferior surface of the clavicle.[5]
It consists of two components: the conoid ligament (posteromedial) and the trapezoid ligament (anterolateral).[5]
Together, these structures suspend and support the shoulder girdle from the clavicle, resist superior displacement of the clavicle relative to the scapula, and provide primary stability to the AC joint.[5] A synovial bursa is frequently present between the two ligamentous components.[5]
Coracoacromial Ligament
The coracoacromial ligament is a sturdy triangular band connecting the coracoid process to the anterior edge of the acromion.[5]
Together with the coracoid process and acromion, it forms the coracoacromial arch, which acts as a protective roof over the glenohumeral joint and the underlying supraspinatus tendon.[5]
A subacromial bursa separates the ligament from the rotator cuff tendons, reducing friction during shoulder movement.[5]
Transverse Humeral Ligament
The transverse humeral ligament spans between the greater and lesser tubercles of the humerus, converting the intertubercular (bicipital) groove into a canal.[4]
Its primary function is to retain the tendon of the long head of the biceps brachii within the groove during shoulder movement.[4]
FAQ’s
The shoulder is composed of three bones: the clavicle (collarbone), scapula (shoulder blade), and humerus (upper arm bone). [1][2] These bones form the shoulder joint complex and collectively enable lifting, rotation, and reaching movements. The shallow socket design of the glenohumeral joint provides the widest range of motion of any joint in the body, but also renders it the most frequently dislocated. [1][3]
The shoulder contains four joints that work in concert to produce smooth, coordinated movement: the glenohumeral (primary ball-and-socket) joint, the acromioclavicular (AC) joint, the sternoclavicular (SC) joint, and the scapulothoracic articulation. [2] Proper coordination across all four articulations is required for full overhead motion and dynamic shoulder stability. [2]
The rotator cuff is a group of four muscles—the supraspinatus, infraspinatus, teres minor, and subscapularis—along with their associated tendons, that collectively stabilise the glenohumeral joint and enable shoulder rotation. [2][5] The cuff maintains the humeral head centered in the glenoid socket during all arm movements. Rotator cuff tears are the leading cause of shoulder pain among U.S. adults. [2]
Common shoulder injuries include rotator cuff tears, glenohumeral dislocations, adhesive capsulitis (frozen shoulder), and glenohumeral osteoarthritis. [1] Shoulder dislocation, the most frequent joint dislocation in the body, occurs when the humeral head is forced out of the glenoid cavity. [3] These conditions affect both athletes and adults over 40 years of age. [1]
Atraumatic shoulder pain is commonly caused by overuse, bursitis, tendinopathy, glenohumeral or acromioclavicular osteoarthritis, or postural strain. [1] Repetitive overhead movements and prolonged seated work postures can progressively stress the rotator cuff tendons and periscapular musculature, resulting in cumulative microtrauma and gradual pain onset. [1]
Frozen shoulder is stiffness and pain that limits shoulder movement.
It develops slowly and can last months to years. It is more common in adults ages 40–60 and people with diabetes.
Shoulder injuries may be reduced through rotator cuff and periscapular strengthening exercises, regular flexibility training, correct posture, adequate warm-up before athletic activity, avoidance of repetitive strain, and use of proper lifting mechanics. [1]
Medical evaluation is recommended if shoulder pain is severe, persists beyond two weeks, or significantly limits daily activities. Swelling, progressive weakness, numbness, or acute pain following a fall or direct trauma require prompt assessment. [1]
References-
- U.S. National Library of Medicine (NLM), MedlinePlus. (2024). Shoulder Injuries and Disorders. A peer-reviewed patient education resource covering common shoulder conditions, anatomy, diagnosis, and treatment options.
Publisher: National Institutes of Health (NIH).
URL: https://medlineplus.gov/shoulderinjuriesanddisorders.html - Miniato MA, Anand P, Varacallo MA. (2023). Anatomy, Shoulder and Upper Limb, Shoulder. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated July 24, 2023.
Indexed in PubMed. PMID: NBK536933
URL: https://www.ncbi.nlm.nih.gov/books/NBK536933/ - Chang L, Anand P, Varacallo MA. (2025). Anatomy, Shoulder and Upper Limb, Glenohumeral Joint. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated March 3, 2025.
Indexed in PubMed. PMID: 30725703
URL: https://www.ncbi.nlm.nih.gov/books/NBK537018/ - Cleveland Clinic. (2024). Shoulder Joint. Comprehensive clinical overview of shoulder joint structure, function, and disorders from a leading U.S. academic medical center.
Organization: Cleveland Clinic Foundation, Ohio, USA.
URL: https://my.clevelandclinic.org/health/body/24780-shoulder-joint - McCausland C, Sawyer E, Eovaldi BJ, Varacallo MA. (2023). Anatomy, Shoulder and Upper Limb, Shoulder Muscles. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated August 8, 2023.
Indexed in PubMed. PMID: NBK534836
URL: https://www.ncbi.nlm.nih.gov/books/NBK534836/ - Cowan PT, Mudreac A, Varacallo MA. (2023). Anatomy, Back, Scapula. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated August 8, 2023.
Indexed in PubMed. PMID: 30285370
URL: https://www.ncbi.nlm.nih.gov/books/NBK531475/ - Hyland S, Charlick M, Varacallo MA. (2023). Anatomy, Shoulder and Upper Limb, Clavicle. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated July 24, 2023.
Indexed in PubMed. PMID: 30252246
URL: https://www.ncbi.nlm.nih.gov/books/NBK525990/ - Mostafa E, Imonugo O, Varacallo MA. (2023). Anatomy, Shoulder and Upper Limb, Humerus. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated August 7, 2023.
Indexed in PubMed. PMID: NBK534821
URL: https://www.ncbi.nlm.nih.gov/books/NBK534821/ - StatPearls Publishing. (2023). Anatomy, Shoulder and Upper Limb, Biceps Muscle. In: StatPearls [Internet]. Treasure Island (FL).
Indexed in PubMed. PMID: NBK519538
URL: https://www.ncbi.nlm.nih.gov/books/NBK519538/ - Wong M, Kiel J. (2023). Anatomy, Shoulder and Upper Limb, Acromioclavicular Joint. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Indexed in PubMed. PMID: NBK499858
URL: https://www.ncbi.nlm.nih.gov/books/NBK499858/ - Epperson TN, Black AC, Varacallo MA. (2023). Anatomy, Shoulder and Upper Limb, Sternoclavicular Joint. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated November 17, 2023.
Indexed in PubMed. PMID: NBK537258
URL: https://www.ncbi.nlm.nih.gov/books/NBK537258/ - Harryman DT, Lazarus MD, Rozencwaig R. (2025). Adhesive Capsulitis (Frozen Shoulder). In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated March 28, 2025.
Indexed in PubMed. PMID: NBK532955
URL: https://www.ncbi.nlm.nih.gov/books/NBK532955/ - Zreik NH, Malik RA, Chaudhry AN. (2016). Adhesive capsulitis of the shoulder and diabetes: a meta-analysis of prevalence. Muscles, Ligaments and Tendons Journal, 6(1):26–34.
PMCID: PMC4915459
URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC4915459/ - Tran G, et al. (2023). Diabetes as a risk factor for the onset of frozen shoulder: a systematic review and meta-analysis. BMJ Open Diabetes Research & Care, 11(1):e003056.
PMCID: PMC9815013
URL: https://pmc.ncbi.nlm.nih.gov/articles/PMC9815013/ - StatPearls Publishing. (2023). Anatomy, Shoulder and Upper Limb, Triceps Muscle. In: StatPearls [Internet]. Treasure Island (FL).
Indexed in PubMed. PMID: NBK536996
URL: https://www.ncbi.nlm.nih.gov/books/NBK536996/
Read More-
Lower Limb
- Complete Guide to Thigh Muscle Anatomy: Learn Parts, Names & Diagram
- Complete Guide on Leg Anatomy with Parts, Functions & Diagram
- Knee Anatomy: Complete Guide to Parts, Names, Functions & Diagram
- Femur Anatomy: Complete Guide with Parts, Names, Functions & Diagram
Upper Limb
- Comprehensive Guide to Arm Anatomy: Parts, Names & Diagram
- Complete Guide to Hand Anatomy: Parts, Functions & Diagram
- Ultimate Guide to Bicep Anatomy: Parts, Names, Functions & Diagram
- Complete Guide to Finger Anatomy with Parts, Names, Functions & Diagram
- Shoulder Anatomy: Ultimate Guide to Parts, Names, Functions & Diagram
- Wrist Anatomy: Ultimate Guide to Parts, Names, Functions & Diagram
- Complete Guide to Nail Anatomy with all Parts, Names & Diagrams
External Sources-
- Wikipedia
- KenHub
- Optometrists
- Cleveland Clinic
- American Academy of Ophthalmology
Official websites of the United States government
- What are the Shoulder Injuries and Disorders?
- What is Dislocated Shoulder?
- How to do Shoulder replacement surgery?
- What is Shoulder pain?
- How to perform Shoulder CT scan?
- How to perform Shoulder MRI scan?
- What is Frozen shoulder? How to take aftercare?
- What is Dislocated shoulder? How to take aftercare?
Medical Disclaimer
All content on HumanBodyPartsAnatomy.com is educational and based on verified, peer-reviewed medical sources. Articles are authored or reviewed by qualified medical or biomedical professionals to ensure accuracy.
This website does not provide medical advice, diagnosis, or treatment. Always consult a licensed healthcare professional for personal medical guidance.
No commercial or promotional interests influence the medical content published on this site.