📅 Published on August 15, 2025 | 🕒 Last updated on January 31, 2026
Overview of Thyroid Anatomy
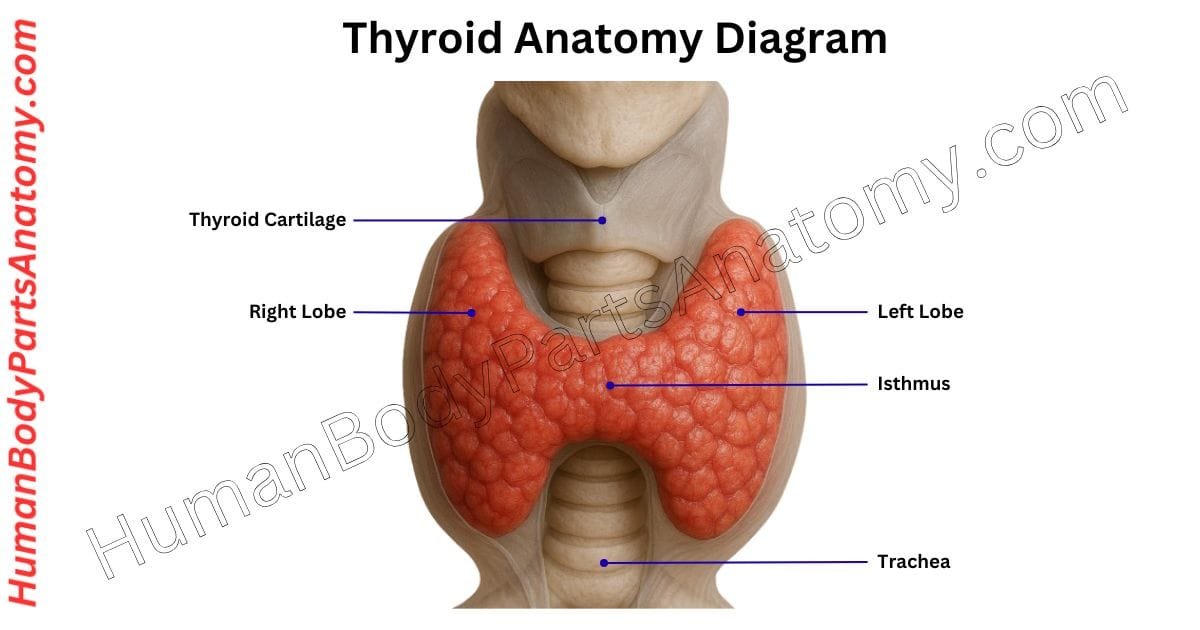
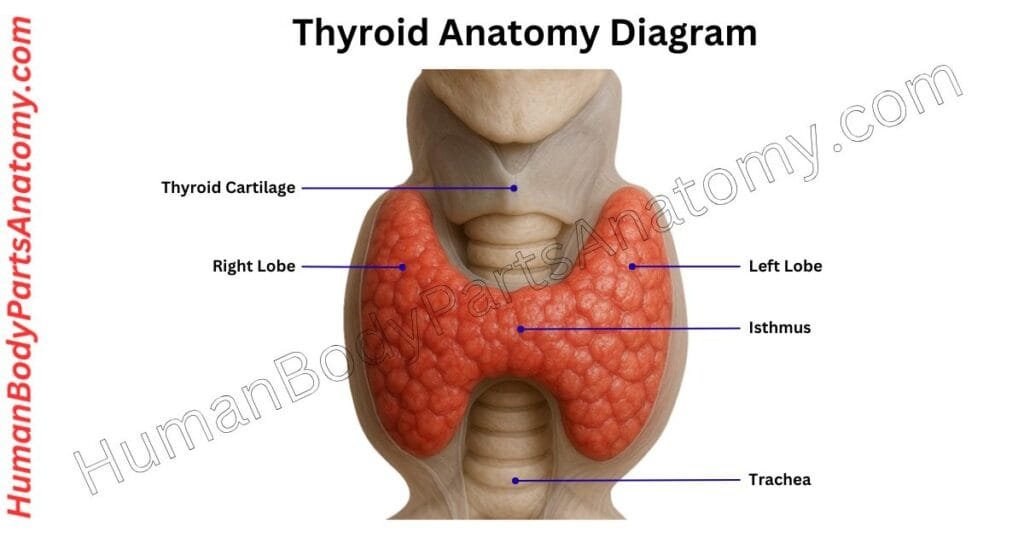
The thyroid gland is a small, butterfly-shaped organ in the front of the neck.[1] It sits in the middle, just over the windpipe (trachea), and stretches from the C5 to T1 vertebrae in the spine.[1] This gland makes important hormones—thyroid hormones (T3 and T4) and calcitonin.[2] These helps control how the body uses energy (metabolism), support growth, and maintain calcium levels in the blood.[2] The thyroid anatomy has two parts called lobes, one on each side of the neck, connected by a thin piece called the isthmus.[1] The isthmus lies over the 2nd and 3rd rings of the trachea.[1] The gland is located behind the sternothyroid and sternohyoid muscles and below the voice box (larynx).[1] On the sides, it is close to muscles and blood vessels, and at the back, it is near the carotid artery and parathyroid glands.[1]
Understanding the thyroid anatomy is essential for diagnosing thyroid disorders and for safely performing surgeries in the neck region.
Anatomy of the Thyroid Gland
Anatomy of Thyroid Gland
- Lobes
- Capsule
- Blood Supply
- Arteries
- Veins
- Nerve Supply
- Microscopic (Histological) Anatomy
- Follicles & Follicular cells
- Parafollicular cells (C cells)
Thyroid Gland Anatomy: Parts & Functions
Lobes
The thyroid gland is a butterfly-shaped gland located in the front of the neck. It has two main parts, called the right and left lobes, which are connected in the middle by a small part called the isthmus.[1]
Sometimes, a small extra part called the pyramidal lobe grows upward from the isthmus.[1] A thin band of tissue, called the levator glandulae thyroideae, may connect the isthmus to a bone in the neck called the hyoid bone.[3]
Each lobe is approximately 5 cm long, 2.5 cm wide, and 2.5 cm thick. The whole gland weighs around 25 grams. It extends from the fifth cervical (neck) vertebra to the first thoracic (upper chest) vertebra.[3]
The lobes go from the middle of the thyroid cartilage (Adam’s apple area) down to the fifth tracheal ring (windpipe). The isthmus is about 1.2 cm in size and lies over the second and third tracheal rings.[3]
In females, the thyroid gland can become slightly larger during menstruation and pregnancy due to hormonal changes.[3]
Each lobe has a cone-like shape, characterized by a top (apex), a bottom (base), three surfaces (lateral, medial, and posterolateral), and two borders (anterior and posterior). The isthmus has a front and back surface, as well as top and bottom borders.[3]
Position of the Thyroid:
- Front side: Covered by skin, fascia (connective tissue), and a thin muscle called the platysma.[1]
- Backside: Close to the thyroid cartilage and the front part of the trachea.[1]
- Side: Near important blood vessels like the external carotid artery and internal jugular vein.[1]
The thyroid gland produces hormones that regulate the body’s metabolism, energy utilization, and growth.[1]
Capsule
The thyroid gland is enclosed by two distinct layers. The inner layer, called the true capsule, is made of strong, flexible connective tissue. Outside this lies the false capsule, which is formed from the pre-tracheal part of the deep cervical fascia.[3]
Just beneath the true capsule is a dense network of small blood vessels known as the deep capillary plexus. During thyroid surgery (thyroidectomy), this vascular layer must be carefully removed along with the true capsule to prevent bleeding and ensure safe gland removal.[3]
Blood Supply
Arteries
The thyroid gland receives a strong blood flow through two main arteries: the superior thyroid artery and the inferior thyroid artery, which supply its upper and lower regions, respectively.[4]
The superior thyroid artery usually branches off first from theexternal carotid artery, near the top edge of the thyroid cartilage. It travels downward, behind the sternothyroid muscle, and reaches the top part of the thyroid.[4] Along the way, it gives rise to several smaller arteries:
- Theinfrahyoid branch (supplies muscles below the hyoid bone),[4]
- The sternocleidomastoid branch (supplies the neck muscle),[4]
- The superior laryngeal branch, which runs with the internal laryngeal nerve through the thyrohyoid membrane,[4]
- And the cricothyroid branch, which connects with its opposite-side counterpart across the midline.[4]
Theinferior thyroid artery originates from the thyrocervical trunk, which is a branch of the subclavian artery. It starts near the edge of the anterior scalene muscle, moves inward, and supplies the back part of the thyroid gland, typically reaching it near the lower third of its outer surface.[4]
A notable branch of this artery is the ascending cervical artery, which should not be confused with the main trunk during surgery due to its similar appearance.[4]
In some individuals (around 10%), an extra artery known as the thyroid ima artery is present. Its origin varies widely—it may arise from the brachiocephalic trunk, aortic arch, common carotid, or other nearby arteries.[1]
Most often, it begins at the brachiocephalic trunk and supplies blood to the isthmus and the front portion of the thyroid gland.[1]
Veins
The inferior thyroid veins usually consist of two veins, but some individuals may have three or even four. These veins begin from a venous plexus on the thyroid gland, where they connect with the superior and middle thyroid veins. Together, these veins help drain blood from the thyroid gland and nearby neck structures.[5]
A key anatomical difference is their drainage pathway. While the superior and middle thyroid veins typically empty into the internal jugular vein, the inferior thyroid veins drain directly into the brachiocephalic veins.[5]
This distinction is important for anatomical study and surgical procedures involving the neck.[5]
The inferior thyroid veins form a venous network in front of the trachea, positioned behind the sternothyroid muscle.[5] From this network:
- The left inferior thyroid vein descends and drains into the left brachiocephalic vein.[5]
- The right inferior thyroid vein travels downward and to the right, crossing over the brachiocephalic artery, and empties into the right brachiocephalic vein near its junction with the superior vena cava.[5]
- In some people, the right and left inferior thyroid veins join to form a single trunk before draining into the right brachiocephalic vein.[5]
Nerve Supply
The thyroid gland lies near two important nerves that come from the vagus nerve: the external branch of the superior laryngeal nerve and the recurrent laryngeal nerve.[1]
These nerves play a key role in voice and breathing. During thyroid surgery (thyroidectomy), there is a risk of injuring them.[1]
If the external branch of the superior laryngeal nerve is damaged, the cricothyroid muscle on that side may become weak or paralyzed. This muscle helpscontrol pitch, so the person may find it hard to change voice pitch or may notice their voice becomes weaker.[1]
Injury to the recurrent laryngeal nerve on one side can prevent the vocal cord on that side from opening properly. This often causes hoarseness and may lead to breathing problems.[1]
If both recurrent laryngeal nerves are injured, the airway can become blocked, making breathing very difficult. In such cases, a tracheostomy (a surgical opening in the windpipe) may be needed to help the person breathe.[1]
Microscopic (Histological) Anatomy
Follicles & Follicular Cells
Each thyroid follicle is surrounded by a thin layer of connective tissue that contains fenestrated capillaries, lymphatic vessels, and sympathetic nerve fibers. These structures support the follicle by supplying nutrients, removing waste, and regulating function.[3]
The follicular epithelium is made up of a simple layer of cells, and its shape changes depending on the follicle’s activity. When active, the cells appear cuboidal to low columnar; when inactive, they become squamous (flat).[3]
These follicular (or principal) cells absorb iodine and amino acids from the blood through their basolateral surface. They use these materials to produce thyroglobulin, a protein rich in iodine that serves as a precursor to thyroid hormones.[3]
This thyroglobulin is stored in the follicle’s central cavity, called the lumen, as a jelly-like substance known as colloid.[3]
In Hematoxylin and Eosin (H&E) stained slides, the colloid stains pink, while follicular cells appear purple. The follicle’s activity can be judged by how the colloid looks:
- Inactive follicles have large lumens filled with dense colloid.[3]
- Active follicles have smaller lumens and less colloid, indicating active hormone release.[3]
Parafollicular Cells (C cells)
Scattered between or around these follicles are parafollicular cells, also called C cells. These cells are part of the neuroendocrine system (specifically, the APUD group – amine precursor uptake and decarboxylation system).[3]
They appear pale or clear under H&E staining and are usually located within the follicular wall but do not project into the lumen. Sometimes, they are also found in small clusters between follicles.[3]
C cells produce calcitonin (thyrocalcitonin), a hormone that helps lower blood calcium levels. It does this by reducing bone resorption (the process of breaking down bone to release calcium) and limiting calcium reabsorption in the kidneys.[3]
FAQ’s
The thyroid gland is a butterfly-shaped endocrine organ in the lower front of your neck, just below the Adam’s apple. It wraps around the trachea (windpipe) and sits in front of the larynx. Its main role is to produce hormones that regulate metabolism and energy use.[6]
The thyroid has two lobes—right and left—joined by a thin bridge of tissue called the isthmus.[1] Some people also have a pyramidal lobe, a normal variant that extends upward from the isthmus.[1] Inside are tiny sacs called follicles that make thyroid hormones.[3]
It produces two key hormones—thyroxine (T4) and triiodothyronine (T3)—that control how fast the body uses energy, affects heart rate, temperature, and growth. It also secretes calcitonin, which helps maintain calcium balance in the blood and bones.[6]
The gland is supplied by the superior and inferior thyroid arteries and drained by thyroid veins.[4] It’s closely related to the recurrent laryngeal nerves, which control vocal cords—so surgeons take great care to protect them during thyroid surgery.[1]
A goiter occurs when the gland grows larger due to iodine deficiency, hormone imbalance, thyroid nodules, or autoimmune diseases like Graves’ or Hashimoto’s. It can cause neck swelling, difficulty swallowing, or a hoarse voice.[7]
The thyroid begins as a small pouch at the base of the tongue and migrates down the neck during early development. Remnants of this path can form a thyroglossal duct cyst or lead to extra thyroid tissue along the migration route.[1]
References-
- National Center for Biotechnology Information (NCBI), National Institutes of Health (NIH). Last review: June 23, 2025. Anatomy, Head and Neck, Thyroid. https://www.ncbi.nlm.nih.gov/books/NBK470452. PMID: 29262169.
- National Center for Biotechnology Information (NCBI), National Institutes of Health (NIH). Last review: February 13, 2023. Physiology, Thyroid. https://www.ncbi.nlm.nih.gov/books/NBK519566. PMID: 30137818.
- National Center for Biotechnology Information (NCBI), National Institutes of Health (NIH). Last review: May 1, 2025. Histology, Thyroid Gland. https://www.ncbi.nlm.nih.gov/books/NBK551659. PMID: 31869123.
- National Center for Biotechnology Information (NCBI), National Institutes of Health (NIH). Last review: July 24, 2023. Anatomy, Head and Neck, Thyroid Arteries. https://www.ncbi.nlm.nih.gov/books/NBK560666. PMID: 32809501.
- Singh, Rajani (2023). “Variations of venous drainage of the thyroid gland and their surgical implications: a narrative review”. Jornal Vascular Brasileiro. 22 e20220163. doi:10.1590/1677-5449.202201632. ISSN 1677-7301. PMC 10153794. PMID 37143504
- Cleveland Clinic. Last updated: June 7, 2022. Thyroid: What It Is, Function & Problems. https://my.clevelandclinic.org/health/body/23188-thyroid.
- National Center for Biotechnology Information (NCBI), National Institutes of Health (NIH). Last update: February 27, 2023. Goiter. https://www.ncbi.nlm.nih.gov/books/NBK562161.
Read More-
Lower Limb
- Hip Bone Anatomy – Complete Guide with Parts, Names, Functions & Diagram
- Complete Guide on Leg Anatomy with Parts, Functions & Diagram
- Complete Guide to Thigh Muscle Anatomy: Learn Parts, Names & Diagram
- Knee Anatomy: Complete Guide to Parts, Names, Functions & Diagram
- Femur Anatomy: Complete Guide with Parts, Names, Functions & Diagram
- Hip Muscle Anatomy – Complete Guide with Parts, Names, Functions & Diagram
Upper Limb
- Complete Guide to Finger Anatomy with Parts, Names, Functions & Diagram
- Complete Guide to Forearm Anatomy: Parts, Names, Functions & Diagram
- Comprehensive Guide to Arm Anatomy: Parts, Names & Diagram
- Comprehensive Guide to Hand Anatomy: Parts, Functions & Diagram
- Shoulder Anatomy: Ultimate Guide to Parts, Names, Functions & Diagram
- Wrist Anatomy: Ultimate Guide to Parts, Names, Functions & Diagram
- Spine Anatomy: Complete Guide with Parts, Names, Functions & Diagram
Human Head
- Skull Anatomy: Complete Guide with Parts, Names, Functions & Diagram
- Ultimate Guide to Eye Anatomy: Parts, Structure, Functions & Diagram
- Tongue Anatomy: Complete Guide with Parts, Names, Functions & Diagram
- Mouth Anatomy: Complete Guide with Parts, Names, Functions & Diagram
- Complete Guide to Tooth Anatomy: Learn Parts, Names & Diagram
- Ultimate Guide to Ear Anatomy: Parts, Structure, Functions & Diagram
- Nose Anatomy: Complete Guide with Parts, Names, Functions & Diagram
Brain
- Parts of the Brain Anatomy: Complete Guide with Names, Functions & Diagram
- Basal Ganglia Anatomy: Complete Guide with Names, Functions & Diagram
- Lobes of the Brain: Complete Guide with Names, Functions & Diagram
- Parts of the Cerebrum Anatomy: Complete Guide with Names, Functions & Diagram
- Midbrain Anatomy: Complete Guide with Parts, Names, Functions & Diagram
- The Cerebellum Anatomy: Complete Guide with Names, Functions & Diagram
Organs
- Kidney Anatomy: Complete Guide with Parts, Names, Functions & Diagram
- Liver Anatomy: Complete Guide with Parts, Names, Functions & Diagram
- Heart Anatomy: Complete Guide with Parts, Names, Functions & Diagram
Medical Disclaimer
All content on HumanBodyPartsAnatomy.com is educational and based on verified, peer-reviewed medical sources. Articles are authored or reviewed by qualified medical or biomedical professionals to ensure accuracy.
This website does not provide medical advice, diagnosis, or treatment. Always consult a licensed healthcare professional for personal medical guidance.
No commercial or promotional interests influence the medical content published on this site.